
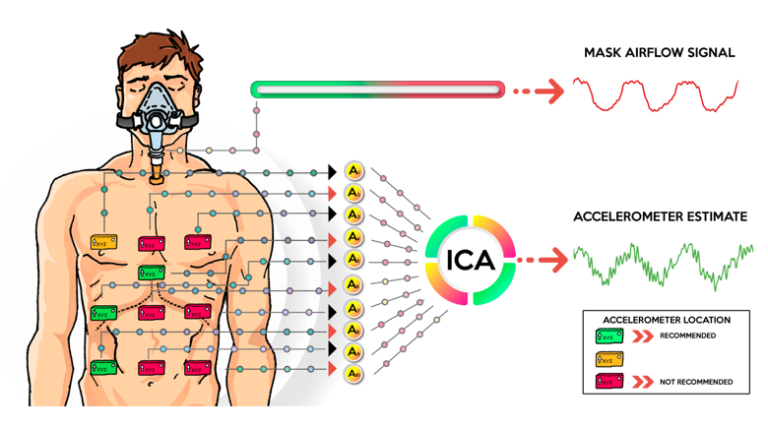
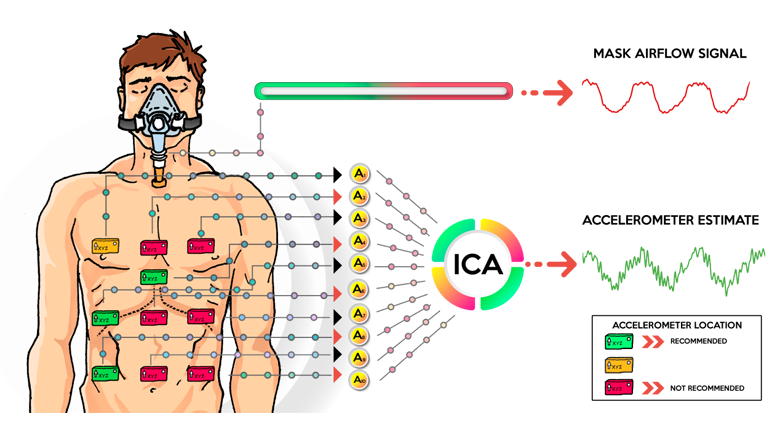
Respiratory rate and phase are important information to assist the assessment of patients’ health in different clinical scenarios. Facial masks are usually employed to record respiratory waveforms, but they cause discomfort and obstruct the breathing of debilitated patients. Accelerometers have been proposed as an alternative to circumvent such drawbacks; however, their best placement and effectiveness in different postures for different subjects were not previously investigated. This work points out the number and optimal placement (on chest and abdomen) of multiple accelerometers to obtain respiratory waveforms. For that, a custom-made microcontrolled system acquired data from thirty male healthy volunteers in three different postures. The sampled data consist of signals from an array of ten accelerometers and an airflow waveform used as reference. The best sensor locations for each posture were identified by optimal linear reconstruction of the reference waveform from the accelerometer data in the minimum mean square error sense. The analysis shows that right-hand side locations contribute more often to optimal respiratory waveform estimates, a sound finding given that the right lung has a larger volume than the left lung. In addition, it is shown that the respiratory waveform can be blindly extracted from the recorded accelerometer data by means of independent component analysis. In conclusion, linear processing of multiple accelerometers in optimal positions can successfully recover respiratory information in clinical settings where the use of masks may be contraindicated. These results open new perspectives for their use in clinical practice and body sensor networks.