
Health care for newborn babies, in particular in a Neonatal Intensive Care Unit (NICU), poses various challenges in defining and coordinating critical decision making processes involving their treatment and the diagnosis of disease. This is primarily due to the fact that there is a significant gap in our understanding of the development of the human brain in its prenatal as well as neonatal stages. Treating a newborn baby is different from treating a child or an adult, and our knowledge of adult and even pediatric medicine is not sufficient for managing these tiny patients. It requires not only developing protocols for facilitating decision making processes in administering nutrition and fluid to neonatal patients, and in carrying out necessary investigations and therapies, but it is also requires that health care providers share experiences and knowledge, thus providing constant review and critical appraisal of practices adopted in a unit. Information processing has a significant role in facilitating this care.
There are various sources of information involving neonatal health care. These include not only our past experiences and knowledge in this domain, but also in the process of treatment, information gathered from daily observation and reports, including different biomedical signals such as ECG, EEG, videos and images, USGs, etc. Even newborn cries can provide a caregiver with cues for effective patient management. At the Indian Institute of Technology (IIT), Kharagpur, we have developed a system (NavajataK) for managing neonatal patients in an NICU in collaboration with the Institute of Post Graduate Medical Education and Research (IPGMER), Kolkata. We also did a few exploratory studies in analyzing newborn EEGs, baby cries, and in developing image and video analysis based systems for neurological examinations. This work was carried out during September 2009 – February 2013 under the sponsorship of the Ministry of Communication and Information Technology (MCIT), Govt. of India. The implementation agency for deploying the system at the Department of Neonatology, IPGMER, Kolkata was Webel Electronic Communication and System (WECS), Kolkata. Some of our significant achievements and outcomes of the project are briefly discussed below.
NAVAJATAK – A web based system for patient management in an NICU
A direct outcome of our project is a secure web enabled system [1] based on a multi-tier architecture for carrying out routine and special operations of a Neonatal Intensive Care Unit (NICU). The system is named NavajataK. It follows a service oriented approach for performing various tasks to coordinate and discharge NICU activities. It includes decision support systems for a number of critical tasks of NICU and also has the modules for managing follow-up patients and carrying out neurological examinations for infants aided by image and video processing tools. The system was operational in the SSKM hospital and during the project period 1,754 newborns were enrolled. Later, three more hospitals, namely M.R. Bangur Hospital in Kolkata, Government District Hospital of Hoshangabad, and Veer Surendra Sai Medical College in Burla were also connected to it.
Video EEG Analysis for detecting newborn epileptic seizure
One of the major components of neonatal care in an NICU is to monitor neonatal EEG signals for identifying neonatal convulsions or seizures. For neonates, epileptic seizures may not have their usual clinical manifestation as observed in cases of infants or adults. Hence, it is of paramount importance to detect these seizures from EEG recordings, which usually cause high energy bursts in the EEG recordings. However, not all these bursts are due to epileptic seizure. There may be various causes for their occurrence such as muscular movement of neonates, power line surges, ocular movement, etc. These noisy bursts are called artifacts.
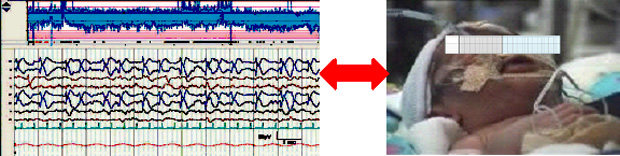
One of the existing solutions to differentiate bursts due to epileptic seizure from the artifacts is the simultaneous recording of video of a neonate and its EEG signal (Figure 1). During the period of burst the doctors also observe whether there is any movement including clinical manifestation in the neonate. This helps in excluding many of the artifacts in the EEG signal. Usually this task is carried out off-line through manual inspection of the recordings. As the neonates are needed to be monitored for a long period of several hours, it requires large storage space in computer disks, as well as many hours of human labor.
In this context, for aiding this inspection we developed a semi-automatic tool for summarizing simultaneous recordings of EEG and video by flagging candidate burst regions and motion segments in EEG and video, respectively. We also improved the burst and artifact detection techniques by choosing suitable features computed from an EEG. These features were selected from a set of features proposed in the past through an empirical feature selection mechanism [2]. We found that features like ratio of mean nonlinear energy, power spectral density, variance and absolute voltage are very effective in discriminating between burst and normal (non-burst) EEG segments. For testing our system, we have formed an annotated data-set, and obtained 78% sensitivity and 72% specificity using a support vector machine (SVM) classifier. These accuracy measures are about 20% higher than those of the reference approaches, reported previously.
Video processing based analysis for neurological examination
It is necessary to carry out different neurological examinations on neonates to assess their stages of development, and treat them accordingly. Not only during their stay at the NICU, but also in their developmental stages as infants up to nine years of age may require being subjected to such tests at a regular interval. There are different protocols that are designed for performing these tests. The Hammersmith Infant Neurological Examination (HINE) chart defines such a set of neurological examinations for assessing infants between 2 and 24 months of age. They include assessment of cranial nerve functions, posture, movements, tone and reflexes. For carrying out these tests, the physicians provide different forms of stimuli to an infant, and observe their postures and behavior. Finally, consulting the HINE chart, they grade the stage of development on a score from 0 to 3.
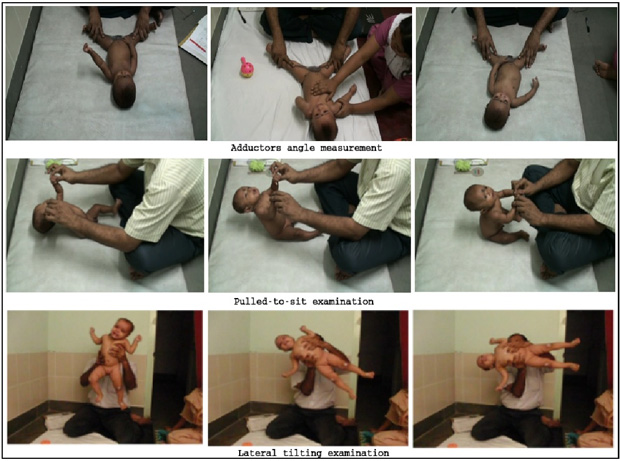
Naturally, assessment based on HINE chart depends on the expertise of the physician. Moreover, some of these tests, such as pulled-to-sit and lateral tilting (refer to middle and bottom rows of Figure 2), are difficult to assess solely based on visual observation. For example, during the pulled-to-sit examination, an examiner pulls the infant by holding wrists and observes the relative movement of the head with respect to torso. It may be difficult for the examiner to follow the head movement from the coronal view. Similarly, in the lateral tilting test, the examiner carries out swift flipping of an infant from left to right (or vice versa) and then observes the simultaneous motion of the movement of hands and legs of the subject. Grading in such cases becomes very much subjective.
Evaluation of human perception of baby cries
There is a popular hypothesis among the scientific community that infants including neonates, who are not at the stages of speaking, communicate their needs and desires by crying. In other words, baby-cries carry a universal language, which may be fundamentally linked with the evolutionary process of a human being. In the literature, there are also reports of various efforts of automated classification of baby cries from their audio recordings. We rather considered testing the hypothesis, whether a human being can interpret baby cries according to their needs. For this we designed a study [4], and collected neonatal cries (for healthy neonates) from the postnatal nursery of the SSKM hospital. In total we have collected 315 neonatal cries, each labeled with four classes, based on their causes observed by the study team, which included master students, nurses and doctors. We could clearly identify three such causes, namely hunger, pain, and wet diaper. The rest of the cry samples were labeled as `others’. We designed a computer based evaluation system for a human participant, who was asked to listen to fifty cry samples, generated randomly, and label them in four of these classes. Before the start of the session, the participant is also asked to go through a training session by listening to a fixed number of samples of cries for each class. There are four categories of participants, including mothers, nurses, doctors, and students / teachers of our Institute. We observed that a significant proportion of participants could classify them into reason based classes. There was a fair agreement among the perception of evaluators supporting the hypothesis on the existence of a perceptible component in the cry signal.
References
- Ray, D.P. Dogra, S. Bhattacharya, B. Saha, A. Biswas, A.K. Majumdar, J. Mukherjee, B. Majumdar, A.K. Singh, A. Paria, S. Mukherjee, and S.D. Bhattacharya, “A Web Enabled Health Information System for the Neonatal Intensive Care Unit (NICU),” Proc. of IEEE World Congress on SERVICES, 4-9 July, 2011, pp.451-458.
- S. Bhattacharyya, A. Biswas, J. Mukherjee, A. K. Majumdar, B. Majumdar, S. Mukherjee, and A. K. Singh, “Feature Selection for Automatic Burst Detection in Neonatal Electroencephalogram,” IEEE Journal on Emerging and Selected Topics in Circuits and Systems, vol. 1, no. 4, 2011, pp. 469-479.
- D. P. Dogra, K. Nandam, A. K. Majumdar, S. Sural, J. Mukherjee, S. Mukherjee and A. K. Singh, “Toward Automating Hammersmith Pulled-To-Sit Examination of Infants using Feature Point based Video Object Tracking,” IEEE Transactions on Neural Systems & Rehabilitation Engineering, vol. 20, no. 1, 2012, pp. 38-47.
- S. Gorain, J. Mukhopadhyay, B. K. Arya, B. Saha, A. K. Singh, B. Majumdar, S. Das Bhattacharya, and A. K, Majumdar, “An Evaluation of Human Perception For Neonatal Cry Using a Database of Cry and Underlying Cause,” Indian Conference on Medical Informatics and Telemedicine (ICMIT-2013), 28-30 March, 2013, Kharagpur, India.