[accordion title=”Introducing Mohamed N. Saad”]
By Max E. Valentinuzzi, maxvalentinuzzi@arnet.com.ar
I recently received an unexpected message from Mohamed N. Saad, out of Cairo, Egypt. Mohamed was submitting an article to be published in IEEE Pulse written about an Arab Muslim, known as Al-Zahrawi (936–1013), a physician and surgeon who lived in Andalucía, Spain. Mohamed was proposing that Al-Zahrawi was an early biomedical engineer.
After reading the article, I was very surprised to learn how much this man, a real scientist, had accomplished, showing creativity, initiative, and a lot of daring and courage. Imagine carrying out surgical interventions of all sorts on patients who were only under the effects of substances like opium (Papaver somniferum), which contains the analgesic alkaloid morphine, or hashish, which is made from the flower of the female cannabis plant, Cannabis sativa. Both substances produce hallucinations or delusions and now are barely considered as painkillers. Remember that real anesthesia was not available until 1846, with a few earlier attempts made by dentists [1]. Another surprise was that Al-Zahrawi can be credited with the first use of syringes, although, according to his account, they were intended only for the urinary bladder and apparently not for the bloodstream—Christopher Wren (1632–1723) is usually recognized for the first use of syringes for that purpose [2], [3].
Mohamed was an assistant lecturer in the Biomedical Engineering Department at Misr University for Science and Technology, Giza, Egypt, where his teaching focused on medical equipment, bioinformatics, clinical engineering, bioelectronics and measurements, digital image processing, and biosignals. He earned his B.S. and M.S. degrees from the Systems and Biomedical Engineering Department, Cairo University, Giza, Egypt, in 2005 and 2011, respectively, and is currently enrolled in the Ph.D. program there. Four years (2006–2010) as clinical engineer in the Department of Medical Equipment Management at the Suez Canal Authority have given him good practical experience. Very recently, he became associated with the Biomedical Engineering Department at Minia University, Egypt. Not long ago, he collaborated with Mabrouk et al. on “Genetic Case-Control Study for Eight Polymorphisms Associated with Rheumatoid Arthritis,” which deals with biomarkers. You can reach him at m.n.saad@ieee.org or m.n.saad@mu.edu.eg.
Acknowledgments
This article was presented during an oral session at the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society held in Milan, Italy, 25–29 August 2015. I must acknowledge the kind assistance and collaboration of Dr. Alex Casson, lecturer with the Sensing, Imaging, and Signal Processing Group in the School of Electrical and Electronic Engineering at the University of Manchester, United Kingdom, who is the speaker, and Dr. Ron S. Leder, chief executive officer and chief scientific officer of RSL Ltd., Mexico, who is an active member of the IEEE History Group. Both investigators have been instrumental in shaping several aspects of this article. Finally, recognition has to be given to the Frankfurt and Istanbul Museums for the History of Science and Technology in Islam. The Istanbul museum has copies of the instruments that are located in the Frankfurt museum, and both museums are run by the same person, Prof. Dr. Fuat Sezgin, who kindly and generously authorized the reproduction of the photos in this article.
References
- H. E. Hoff, “Dentistry and the centenary of anaesthesia,” McGill Dental Rev., vol. 9, no. 1, pp. 18–30, 1947.
- M. E. Valentinuzzi. (2011). Anticoagulants: An essential transfusion component—How they came about. IEEE Pulse, 2(2), 45–50.
- M. E. Valentinuzzi. (2011). The development of transfusion: Techniques and technology. IEEE Pulse, 2(3), 71–75.
[/accordion]
In one’s career, it is good to look back at the predecessors in the field. Biomedical engineering history is full of hidden treasures, one of whom is Al-Zahrawi, a Muslim surgeon who had a wide reputation in Europe during the Middle Ages. Herein, besides recalling that he was a surgeon, the intent is to spotlight his talent in biomedical engineering. Important contributions in surgical instruments come up readily in a review of his work, contradicting the view some have maintained of him as a mere compiler. He was a true inventor, creating many surgical instruments that were not known in the Greco-Roman era. Quite early, he produced contributions influencing surgical procedures in Europe from the 14th to the 18th centuries. As a problem solver, he was aware of anatomical and physiological problems, and he moved through design, methods of manufacturing, and practical applications. The illustrations of such instruments in his encyclopedic work, Al-Tasrif, reflect his willingness to teach.
Background
Biomedical engineering applies a variety of concepts to solve medical and biological problems, and it is currently divided into many subdisciplines [1], [2]. Studying its history is beneficial as it frees the mind from the narrow, static images of the past sometimes imposed by the new and modern concerns. Exposure to the history of science enables students to think, ask questions, explore concepts, and understand what science is about and how it is conducted [3], [4].
Although biomedical engineering as a dedicated field has only recently become a staple of university curricula and departments, biomedical technologies have a very long history. Researchers have discovered in Mehrgarh, Pakistan, 11 drilled teeth belonging to nine adults. These represent the earliest known ancient dental procedures, dating back to ca. 7000–5500 B.C. [5]. It is argued that the first prosthetic limb in the world was discovered in Egypt in 2000 by German archeologists. A mummy, dating back to ca. 1000 B.C., was uncovered in Thebes, and its big toe had been replaced with a wooden prosthetic, which was tied to its foot [6]. Also in Egypt, hollow reeds were used to investigate the function of human internal organs ca. 1000 B.C. [7].
In Mexico, the Maya and Aztecs fixed dental cavities with mechanical tools from the 10th century through the 14th century. In addition, they manufactured the first sanitary sewage system in the Americas. Mexicans used the digitalis tree to treat arrhythmic disorders and discovered the medical uses of a variety of other plants [8].
In the 19th century, physiologists and physicians invented medical instruments to help patients and to examine the laws of nature. The 20th century saw the start of the full flowering of biomedical engineering’s progress [9]. There are still many gaps to be filled in the study of biomedical engineering history. This article provides an overview of Al-Zahrawi’s contributions, so as to fill at least one of those gaps.
Al-Zahrawi’s Biography
Al-Zahrawi (936–1013 A.D.)—whose full name was Abu Al-Qasim Khalaf ibn Abbas Al-Zahrawi and who was known as Abulcasis, Albucasis, Zahravius, and Az-Zahrawi for short—was named after Al-Zahraa, a city near Córdoba, Andalucía, Spain, which was the summer residence of the Umayyad caliphs; it was where he was born and died. A street in Córdoba (where he lived) carries his name, Albucasis. Of Arab descent, his roots can be traced to Al-Madinah Al-Munawwarah, Saudi Arabia [10]–[14].
As an example of his humanity, Al-Zahrawi spent half of his working hours treating patients as an unpaid volunteer [11], [15]. He recommended that students with high grades in language, grammar, mathematics, astronomy, and philosophy be eligible to study medicine [16]. The relationship with his students was like that of a father and his children. He advised his students to specialize in one field of medicine so as to achieve proficiency, and he always showed that he valued ethical concepts. Often, he made references to Galen, Paul of Aegina, Al-Razi, and ibn Al-Jazzar [14], [17].
Al-Tasrif is the only known book by Al-Zahrawi. It consists of 30 treatises that contain topics from a variety of medical branches. It was considered a reference manual for physicians in Europe during the middle ages [17], [18]. Written over a span of approximately 50 years, it reflects Al-Zahrawi’s medical practice, research, teaching, and experiments and shows a number of advanced medical techniques and tools. Al-Zahrawi elaborated on the treatment of a dislocated shoulder, later known as Kocher’s method. He described a position for fetus delivery, later termed the Walcher position. He detailed the method of ligaturing blood vessels about six centuries before the French surgeon Ambroise Paré. The last treatise in the book is related to surgery and comprises about 200 illustrations of surgical and medical instruments and devices, most of which were invented by Al-Zahrawi himself [10], [19].
Contributions in Obstetrics and Gynecology
![Figure 1: Vaginal speculums [23]: (a) Al-Zahrawi’s design and (b) and the ancients’ design. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope01-2516180.jpg)
Al-Zahrawi used a vaginal speculum to help in the extraction of a dead fetus [Figure 1(a)]. The two-blade speculum (dilator) resembles a book press and is equipped with a screw arrangement for unscrewing its spoon-like branches to widen the genital tract. The two screws are finer than those of the press. The screws are produced from ebony, ivory, or box-tree wood. The distance between the branches is widened or narrowed depending on the screws’ direction of rotation [20]–[23].
He specified the dimensions of each speculum’s woody base as a length of one and a half spans (about 33 cm, if we recall that a span is the distance measured by a human hand, from the tip of the thumb to the tip of the little finger), a width of 2 in, and a thickness of 1 in. Additionally, he specified that the branches’ lengths should be comparable to the vaginal depth, about half a span (11 cm) or a little more. In case the branches were longer than the vaginal depth, he suggested adding folded pads to the branches’ contacts to avoid inserting the full length of the branches [22], [24].
![Figure 2: A cephalotribe with curved jaws [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope02-2516180.jpg)
Also, the speculum could be used in removing abnormal enlargements in the womb. After applying the speculum, a broad scalpel (Arabic: nashl) was used to incise the swellings. Al-Zahrawi’s speculum is clearly different from those of the ancients (Archigenes and Soranus of Ephesus) in both the used materials and the principle of action, as shown in Figure 1 [26], [27].
Al-Zahrawi was the first surgeon, before the famous Chamberlen family, to use a cephalotribe (Arabic: mishdakh), which was a type of crude forceps (Arabic: kalaleeb). The cephalotribe has saw-toothed curved jaws and very strong handles, as shown in Figure 2. Also, he described another type of cephalotribe (scissors) that has straight jaws (Figure 3). The later looks somewhat like the modern cranioclast [22], [23].
![Figure 3: A cephalotribe with straight jaws [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope03-2516180.jpg)
Al-Zahrawi used a hook with two horns (Arabic: sinnarah that al-shaukatain) for the extirpation of a dead fetus from the uterus. The horns are sharp and curved away from each other. They are connected to a thick handle to avoid damage to the hook when extracting the fetus, as shown in Figure 4 [22], [23], [27]. He was a pioneer who used a glass mirror to reflect sunlight to inspect the uterine cervix [28].
![Figure 4: A hook with two horns for the extraction of a deceased fetus [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope04-2516180.jpg)
Contributions in Urology
Al-Zahrawi’s contributions were a cornerstone in the evolution of urology science. He was considered the founder of lithotripsy by Spink and Lewis [29] as well as Kirkup [30]. The forceps, drill (Arabic: mithqab), scalpel, and metal probe (Arabic: mirwed) were all Al-Zahrawi’s innovations used in lithotripsy, and they reduced the risks associated with of bladder stone surgery.
The forceps were used to crush large stones inside the patient’s bladder so as to gradually move them out: they were like a primitive lithotrite. A modification of Al-Zahrawi’s forceps was made by Andreas A. Cruce in the 18th century when he replaced the manual compression on the handle with a screw action. In the 19th century, Heurtloup modified Al-Zahrawi’s lithotrite by replacing the jointed saw-toothed blades with separated parallel blades [13], [14], [31].
The drill was an instrument used to make holes in the small stones that remained and moved toward the penis, blocking the flow of urine. It was made of Damascene steel, with a sharp triangular end and a wooden handle. Al-Zahrawi rotated the small drill with his hands to pierce the stone; thus, the stone could be extracted, and the bladder could be irrigated [14], [22], [32]. Rigal de Gaillac, Fournier de Lempdes, and Franz von Gruithuisen used drills that were very close in shape to Al-Zahrawi’s drill. In the 19th century, Al-Zahrawi’s drill was replaced by a rotating wheel introduced by Leroy d’Ettiole and Jean Civiale [31], [33].
The metal probe was a diagnostic tool used to confirm the presence of stones inside the relatively large bladder cavity before the start of a perineal cystolithotomy operation [14], [31]. The scalpel was introduced by Al-Zahrawi in lithotripsy as a tool to make an incision in the area between the anus and the testicles. It differs from the scalpel introduced by Meges of Sidon in the first century, which had two sharp cutting edges. The upper edge is not sharp but wide and thick, letting the surgeon exert pressure on it, while the lower edge is in the shape of half circle and sharp for cutting purposes. Marianus Sanctus and Shelsden used scalpels that resembled Al-Zahrawi’s design [31], [33].
![Figure 5: A straight catheter for urinary bladder irrigation [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope05-2516180.jpg)
A trailblazer in urology, Al-Zahrawi also produced a catheter. This catheter is straight compared to the S-shaped catheter introduced by Galen [37]. Al-Zahrawi’s catheter consists of a silver tube with a tiny funnel end. The tube is narrow, smooth, hollow, and long (about one and a half spans—33 cm), as shown in Figure 5. The tube was lubricated before being inserted in the male urinary tract. A double thread was used to hold a piece of cotton or wool that was inserted in the beaker-like end of the catheter. After reaching the bladder, the cotton or wool plug was withdrawn through the tube to irrigate the bladder [22], [23].
Al-Zahrawi also invented a syringe long before Christopher Wren’s (1632–1723) attempts [34]. His syringe (Arabic: zarraqah), made of silver or ivory, consists of a long narrow cannula and a broader straight cylindrical barrel and copper piston, as shown in Figure 6. The cannula’s end contains three perforations, and its diameter corresponds to the width of the urinary tract. Like today’s syringes, the piston is pressed to deliver medications in liquid form to the bladder. The plain syringe (that is, with a plain tip that slips over the needle hub) was used for the injection of medications to treat ulcers, blood clots, or pustules in the urinary bladder [22], [23].
![Figure 6: A plain syringe for the injection of medications in the urinary bladder [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope06-2516180.jpg)
Al-Zahrawi described another syringe (Arabic: mihqan), which was used to evacuate the hydrocele [32]. This syringe has a balloon-like hose instead of the piston, as shown in Figure 7. The hose is tied to the shaft with a strong piece of cord [23].
He was the first to describe penile fracture, managing the painful event by introducing the penis into a goose’s neck or a cannula. Thereafter, the penis was wrapped and bandaged [35].
![Figure 7: A balloon syringe for hydrocele evacuation [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope07-2516180.jpg)
Contributions in Pediatrics
Al-Zahrawi used scissors (Arabic: miqass) in the circumcision of boys. The shape of the scissors is flattened, sharp, and straight, with the pivot tempered. The handles and the blades of the scissors are equal in length to provide the fingers holding them with the correct sensation (Figure 8). Surgical scissors are an Arabian invention speculated to be by Al-Zahrawi as they were not described elsewhere before his work [11], [13], [14], [21].
![Figure 8: A pair of surgical scissors used in the circumcision of boys [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope08-2516180.jpg)
A ring-shaped cautery was used to treat the area around the lumbar vertebrae (Figure 9). This area of a child’s body is associated with back pain associated with the spinal column. Another cautery was applied to treat the superficial area around the sciatic nerve. It resembles the previously described cautery except that it has more rings with smaller diameters connected to each other, as shown in Figure 10 [23].
![Figure 9: A ring-shaped cautery used in the treatment of the lower area of lumbar vertebrae in children [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope09-2516180.jpg)
![Figure 10: A cautery for the treatment of the superficial area around the sciatic nerve [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope10-2516180.jpg)
A scalpel was used in infantile hydrocephalus surgical operations (subdural and subgaleal effusions). The function of the scalpel is to open the anterior fontanelle and evacuate intracranial fluid [36]. Another scalpel type was applied for a deeper, T-shaped incision when the fluid had accumulated between the bone and the meningeal coverings [37]–[39]. An extremely fine scalpel was introduced to enlarge the meatus in the case of hypospadias or meatal stenosis.
Al-Zahrawi used a slim lead cannula in the meatus to keep it opened [13]. His procedures were the same as those of Paul of Aegina and Galen, with the preference of a lead tube instead of a solid rod [11]. In case of nasal polyps, a thick, knotted linen thread was applied by inserting it into the nose with a probe until it came out through the mouth, removing the polyp with a hook [11], [16], [21]. A hook and a fine scalpel removed early-stage cysts beneath the tongue [11], [40]; thereafter, the wound was cauterized [13], [40]. Bulb syringes delivered enemas to children [21], [41]. Al-Zahrawi recommended cauterization for harelip followed by suturing the edges together. Essentially the same technique continued until the 18th century [42].
Contributions in Cauterization
Al-Zahrawi greatly expanded the field of cauterization. He used more than 50 types of cauteries (metals and caustic drugs) for the treatment of various diseases [39], [43] and explained the advantage of using hot metal cauteries over caustic drugs, pointing out that the neighboring tissue is inevitably damaged when using the latter [25].
The shapes of the cauteries invented by Al-Zahrawi were appropriate for the target parts of the body. The cautery used for backaches and headaches looks like a nail, the one used for narrow places is pointed, and the one for the nose looks like a saw [13], [25]. He created a cautery (Arabic: mikwah zaytuniyah) for the treatment of epilepsy and hydrocephalus that is made of iron. It looks like an olive pit, as shown in Figure 11. The shape of the cautery used in dropsy looks like a beak; it was applied vertically to allow fluid outflow. Al-Zahrawi used ink to mark the precise place for cauterization [43]. The shape of the cautery in the case of a harelip resembles a knife [11], [13]. The first notice and description of hemophilia was credited to Al-Zahrawi, who recommended cauterization until bleeding, if present, stopped [44].
![Figure 11: An olivary-shaped cautery used for hydrocephalus [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope11-2516180.jpg)
Al-Zahrawi’s predecessors touted the superiority of gold as the best material for cauteries. On the contrary, he demonstrated the disadvantages of using gold for cauteries. His criticisms included the following:
- Gold may sometimes liquefy due to overheating.
- The right degree of heat that should be transmitted to gold cannot be ascertained due to its reddish color.
- Gold cools down very quickly.
He pointed out that iron is better than gold in cauteries [11]. His preference for iron is in line with modern knowledge, as the melting point of iron is 1,535°C, while that of gold is 1,063°C [29]. This recommendation reflects his keen experimental observations [43]. He discussed the appropriate amount of iron heating, underlining that its color changes to red, then to white. He also explained the use of red-hot iron (not white-hot iron) because the former coagulates the tissues, while white-hot iron splits as a blade [25], [45].
Contributions in Fractures and Dislocations
![Figure 12: A saw for connecting holes in the case of hairline fractures of the skull [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope12-2516180.jpg)
Al-Zahrawi diagnosed hairline fractures of the skull by shaving the scalp and spotting it with ink—this made the thin linear fracture visible. He dealt with the small fractured bones using a nonsinking trephine, a saw (Arabic: minshar), appropriate forceps, and a chisel. Trephines with different depths to fit the patient´s skull thickness were used, including a circular margin as safety procedure. The distance between the apertures, made by the trephine, was about the thickness of a probe (about 7 mm). Sharp iron saws connected the apertures with handles made of box-tree wood and almost circular blades (Figure 12). Larger saws were used in case the small, fine saws were ineffective. Al-Zahrawi noted that the surgeon should use tremendous delicacy to prevent the penetration of the duramater by either the trephine or the saw. After removing the depressed bones with forceps, he used a slender chisel to smooth the roughness in the circular margins of the penetrated skull bone [39], [46]. Guy de Chauliac followed the procedures of Al-Zahrawi by avoiding direct circular trephination [47].
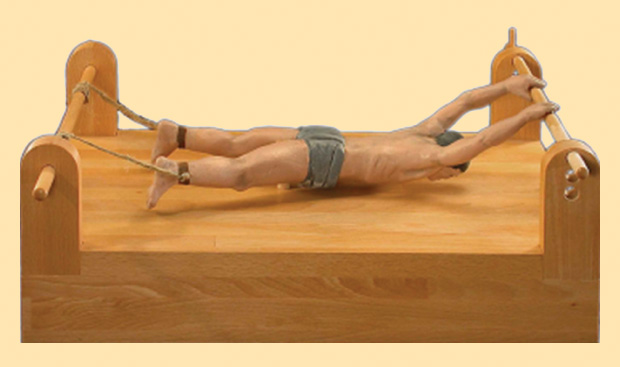
In case of inner nasal fractures, he applied a cloth in each nostril to keep the fractures in the correct position. The cloths were shaped like wedge tents and made of twisted linen [13]. He invented a wooden orthopedic bench to extend limbs in the treatment of dislocations of the dorsal vertebrae and limb fractures (Figure 13) [15], [23].
Al-Zahrawi invented different types of splints (Arabic: jabira) for simple and compound fractures. The trapeze splint was used for reducing fractures of the humerus. The splint consists of a smooth, thin stick in the shape of a bow with two strings, each attached to one end of the stick. Ball splints were used for small hand fractures, while pestle splints were used for reducing shoulder dislocations [15], [48]. He added egg and flour to a plaster for shoulder immobilization [15], [17], [25], [48]. He treated the fracture of the femoral shaft with the knee in flexion using a coaptation splint [49].
Contributions in Ear, Nose, and Throat Treatment
![Figure 14: A guillotine for removing swollen tonsils [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope14-2516180.jpg)
Al-Zahrawi used a tongue depressor, a hook, and a guillotine to remove swollen tonsils [25]. The tongue depressor (spatula) was thin and made of silver or bronze; it was used to hold the mouth open. The hook was used to hold on to the tonsil during the dissection process. The guillotine was made of hardened iron or steel and resembled a pair scissors but with transverse sharp extremities, as shown in Figure 14. If this kind of guillotine was not available, he proposed the use of a curved scalpel, which has a sharp concave side and a blunt convex side. The same instruments and procedures could be used to cut off a pale and elongated uvula or to excise throat tumors [21], [26], [50], [51]. Kirkup supposed that Al-Zahrawi’s guillotine was the first type of surgical scissors [52].
The tongue depressor could also be used to extract a foreign body from the throat and esophagus by keeping the tongue immobilized to widen the field of view as much as possible. In cases when the foreign body was still invisible, a gatherer was used. The gatherer is made of lead and just thicker than a probe (about 7.1 mm) [16]. It is shaped like a pair of scissors with a curved, sharp, rough end, as shown in Figure 15. Al-Zahrawi inserted the gatherer gently into the patient’s throat while the patient’s head was tilted backward. He pushed the gatherer down until the foreign body was caught up by the gatherer. Then, he pulled the gatherer until the foreign body was removed from the throat. He noted that the physician should use tremendous delicacy to prevent touching the larynx as it might cause coughing. Also, he recommended that the patient be the one to introduce the gatherer into the throat (under the supervision of the physician) as the patient knows better the exact place of the obstruction [51].
![Figure 15: A gatherer with curved extremities for extracting a foreign body from the throat and esophagus [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope15-2516180.jpg)
In case of thyroid tumors, Al-Zahrawi described how to make punctures of the gland with an instrument that looks somewhat like the modern aspiration needle. This technique was used to differentiate among different types of goiters [53]. He used a pointed cautery to treat otalgia (earache). Several points on the auricle were cauterized [43]. He used a fine scalpel (Arabic: mibdaa raqiq) to crush a foreign body that had entered the ear and swollen up inside due to moisture [23]. A plunger-controlled syringe was invented to introduce medications into the ears [15], [22]. He used tweezers (Arabic: gift) to get rid of any foreign bodies from the auditory canal (Figure 16) [16], [23]. Foreign bodies were sucked out by a metal cannula from the external ear [54]. This cannula was also used to prevent the damage of the surrounding tissues in the throat or the mouth in case of cauterization [35].
![Figure 16: Tweezers for removing foreign bodies in the auditory canal [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope16-2516180.jpg)
Contributions in Opthalmology
Al-Zahrawi used a needle, a horse-tail hair, and a sharp, smooth blade, along with a scalpel (Arabic: mibdaa) in the treatment of pterygium (Arabic: azzafra), the growth of pink, fleshy tissue on the white of the eye, or conjuctiva. The needle was inserted under the pterygium to raise it. Then, the horse-tail hair was inserted under the needle to saw off the pterygium outside the cornea. Horse-tail hair was used because the technology of the era was unable to produce a man-made instrument of the desired thickness and sharpness. In fact, a recent study has shown that the thickness of a horse-tail hair is about 0.2 mm and recommends its use in ophthalmic surgeries [73]. The blade was used to raise and pick off the pterygium and to cleave the adhesions of the eyelid. Al-Zahrawi used the scalpel to remove adhesions in the inner corner of the eye and to cut off pterygium [23], [25].
He described a crescent-shaped cautery for use when the eyelashes grew turned into the eye. The roots of the hair on the eyelid were cauterized to stop corneal irritation [13], [23]. The same cautery was applied for the relaxation of the upper eyelid. The required length of cauterization was the length of the eyelid. The required thickness of cauterization was one-third the thickness of the skin. Al-Zahrawi noted that the physician should use tremendous delicacy to prevent burning the temples [13], [74]. He used an eye speculum with three pin-shaped projections for holding up the upper eyelid while cauterizing. Olive oil was added to the contacts of the projections to prevent eye damage [13].
![Figure 17: A couching needle for the treatment of cataracts and hypopyon [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope17-2516180.jpg)
He used a probe, one or two small hooks, and a small spear in the treatment of symblepharon (Arabic: iltisaq), i.e., adhesion of the eyelids to the eyeball. The tip of the probe or the hook was used in the eversion of the eyelid. The spear was used to incise the sebaceous cyst and clear off the adhesions [13]. He used a couching needle (Arabic: miqdah) in the treatment of cataracts and hypopyon (inflammatory cells in the anterior chamber of the eye). The needle has a small pointed end, as shown in Figure 17 [15], [23], [25]. A special surgery needle was used instead of the couching needle if the eyeball was resistant to insertion [56].
Contributions in Dentistry
![Figure 18: A hook for lifting broken teeth that cannot be extracted with tongs [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope18-2516180.jpg)
Al-Zahrawi used several types of tongs for removing teeth and tooth fragments. He used tweezers to extract the roots of teeth and jawbone fragments. He used a hook to lever out broken teeth that could not be extracted with the tongs (Figure 18). For removing tartar, he employed a variety of raspatories (Arabic: mijrad), instruments for scraping and smoothing the teeth (Figure 19). He was aware that tartar accumulates on the teeth and causes gingivitis and periodontal disease [15], [40]. In cases of gingivitis, gingivectomies were performed using a cautery. The shape of the cautery resembles a small scalpel, sharp and pointed to the gum tissue. This cautery functioned as a modern electric scalpel does today [40].
Al-Zahrawi recommended fixing loose teeth to their sound (permanent, natural, and healthy) neighbors using a gold or silver wire. He preferred gold wire as it does not corrode [57]. He proposed the use of prosthetic dentures made of animal bones for replacing missing teeth [16], [26], [40]. He treated epulis (oral fistulae) by ablation using a hook or forceps followed by the use of cautery or curette [25], [40], [43]. He was a pioneer who depicted dental arches [10] and treated deformities of the mouth [45]. He used minerals in oral and dental diseases, including alkali (sodium carbonate and potassium carbonate), alkyonion stone (silica crystals, calcite, and collagen), alum (hydrated potassium aluminium sulphate), bitumen, cooked clay (phyllosilicates), arsenic, sulfur, Armenian bole (red clay), borax (sodium borate), lime, verdigris (copper acetate), coral (calcite), lapis lazuli (lazurite), marcasite (pyrite, an iron sulfide), marble, nacre, orpiment, salt (halite), and vitriol [58].
![Figure 19: Raspatories for removing tartar [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope19-2516180.jpg)
Aneurysm Treatment
Al-Zahrawi invented the aneurysm needle [25]. For migraine headaches, pain in the temporal muscles, and other chronic headaches, he suggested shaving the affected area and making an incision using a knife. Then, he used a hook’s tip to twist and cut the superficial temporal artery. The hook could have one, two, or three prongs. Then, he used an aneurysm needle and a thread made of silk or lute-string to ligate the artery and control blood flow. He provided this treatment in addition to cauterization by a metal double-bladed cautery [39], [46], [59].
When enlargement of an artery at the mouth occurred, Al-Zahrawi suggested using a knife to make a longitudinal incision at the affected area. He used hooks to widen the field of view to simply canvass the artery. Then, he used an aneurysm needle and a double thread to tie the artery in two places. A scalpel was used to open an aperture between the two ligatures to let out the infected blood [60]. As a disinfection procedure, he recommended the use of medical packs until the ligatures fell away [21].
Contributions in Bleeding Control and Wound Healing
Al-Zahrawi was the first to use cotton to control bleeding. He also developed the plaster (gypsum, a soft sulfate mineral) used for fractures, as well as the adhesive bandage (sticking plaster) used for simple injures. These contributions are still universally used in health care facilities [14], [21], [61]. He suggested digital pressure, cautery, ligature, dry dressings (cotton or linen), or cold water to control bleeding [25], [59]. He recommended that bandages be made of soft linen and wrapped less tightly with increasing distance from the site of injury [48].
He used linen towels saturated with alcohol and rose oil along with wax to stop hemorrhage during diagnosis and to minimize infection after surgery. Then, he healed the wounds with towels soaked with basilicon ointment (the name given to various ointments that were believed to have special virtues or properties, e.g., as suppuratives) [39]. The advantages of linen as a surgical dressing include that it helps in tightening wounds, drying up sores, keeping the skin from sweating, and allowing ventilation of the wound without polluting it. Alcohol is an antiseptic, hemorrhage stopper, and dryer. Rose oil helps grow flesh in deep wounds, calms painful sores, and constricts and cools wounds. Basilicon ointment saves the wound from ulcers and putrefaction [62].
He used cotton dipped in saline water and wet cotton that had been heated under the sun for the sterilization of wounds after cauterization. In cases of oral fistulae, warm saline for sterilization was advised.
In cases of opening up of swellings occurring in the womb, a dressing soaked in rose or green oil with styptics (a specific type of antihemorrhagic agent that works by contracting tissue to seal injured blood vessels) was placed on the wound after its evacuation. Liquorice and aristolochia were used as wound coolers and for their anti-inflammatory effect before the application of ointment [62].
For nasal polyps, Al-Zahrawi inserted a lead tube into the nostrils as a postoperative treatment. The lead tube was loaded with Egyptian oil or drying medicaments by instillation for the complete healing of the wounds. During the surgery, he recommended the use of vitriol in case of bleeding. As a sterilization procedure, the patient was asked to rinse his or her mouth out with salt and vinegar [11], [40].
As hemorrhage was inevitable in gynecomastia surgery, Al-Zahrawi recommended digital pressure and cotton packs to stop bleeding. He was the first surgeon to employ styptic powder after a severe gynecomastia surgical treatment. The components of the styptic powder are listed in Table 1 [63], [64].
[accordion title=”Table 1. Natural Substances and Their Effects in the Surgical Management of Gynecomastia, as Described in Al-Tasrif”]
| Common Name | Scientific Name | Effects |
|---|---|---|
| Dragon’s blood | Calamus draco | Wound healing, antimicrobial |
| Sarcocolla | Astragalus fasciculifolius | Wound healing |
| Myrrh | Commiphora molmol | Wound healing, antibacterial |
| Aloe | Aloe vera | Wound healing, antimicrobial |
| Gum Arabic tree | Acacia Arabica | Antibacterial |
[/accordion]
He recommended that the patient should gargle with vinegar and cold water after tonsillectomy surgery. In case of hemorrhage, the patient was asked to gargle with water in which pomegranate rind or myrtle berries had been boiled, and styptic powder was also used [26]. Pomegranate rind and myrtle berries were used for agglutinating of wounds and stopping hemorrhage [62].
Contributions in Surgical Suturing
Al-Zahrawi was the first surgeon to use animal gut to suture a wounded intestine. He understood that a compatible biomaterial should be used inside the human body so that the body would not reject it [11], [46], [65]. He recognized that animal gut is a dissolvable material after he discovered that a monkey had eaten the strings of his lute—he checked the monkey’s excreta but did not find the lute strings. Suture strings are still made of animal gut today [15], [61]. Other suturing materials included flax, horse hair, silk, and wool. In addition, he used giant ants in abdominal suturing. The ant was left to bite the wound edges. Then, the ant’s head was separated from its body, acting like modern Michel clips [17], [66].
Contributions in Cosmetology
Al-Zahrawi dedicated Chapter 19 of his Al-Tasrif to cosmetics, which he considered a medical branch, naming it “the medicines of beauty” (Arabic: adwiyat al-zinah) [17]. In dentistry, he discussed teeth whitening and gum strengthening. The chapter includes discussions of hair-removal sticks and hair dyes as beauty tools. He discusses lotions to straighten curly hair as well as suntan lotions, along with their ingredients. He describes incense, scented aromatics, and perfumes that were rolled and pressed into sticks, which looked somewhat like today’s roll-on deodorants. He also invented perfumed sticks, rolled and pressed in a mold (Arabic: lafayif), which are the earliest antecedents of modern solid deodorants and lipsticks [65], [67].
Contributions in Pharmacology
Al-Zahrawi was concerned with the delivery of the right dose of a mixture of powdered drugs to the patient. He was aware of the suspension property of the powder mixtures that would deliver incorrect dosages. Also, he considered powders less stable than tablets as the former have more surface area exposed to air. Powders are easily penetrated by air, which accelerates their deterioration. Tablets are easier to use while traveling or at home [68]. So he fabricated tablet molds for single doses of powdered medicines.
The plate used in tablet mold manufacturing was made of hard, smooth wood, ebony or ivory, or a grinding stone. Its length is 9 in (or fingers, an ancient unit of length), with a width of 1.5 in and a thickness of 2 in. The plate was cut horizontally in two halves and engraved with the intended number of circles on each side in the appropriate size and shape for the desired tablets. Each engraved circle was half the height of the tablet. A mirror image of the relevant name of the tablet was engraved on one side of each mold so the tablets could be easily distinguished from one another. He was the first to print the name of the drug on the tablet.
To ensure that the mold would not stick or disintegrate, it was painted with oil (Arabic: duhn) before its closure. Al- Zahrawi added gums (such as acacia and tragacanth) to the tablets as preserving agents. He described the testing procedures required to obtain the exact weight of the produced tablet. The raw material was inserted into the mold while soft. Then, the material was weighed. If it was lighter than the required weight, the engravings were widened. The procedure was repeated until the material reached the desired weight [17], [65], [68].
Al-Zahrawi used silver foil to store single doses of powdered medicines. He also wrapped single doses of drugs in catgut packs, which were ready for swallowing. The packs would dissolve, releasing the medications inside the stomach. This procedure was unmodified until the creation of modern drug capsules [65].
He was aware of the concept that a drug may be substituted due to cost or availability. He indicated that the effective weight of a dose of a drug might equal half or double the weight of a dose of an alternative. He studied the weights and measures used by the Greeks and the Egyptians, as well as what was used in the Eastern Caliphate and Spain. In his weight measurements, he used ratl, ouqiyah, mithqal, and dirham, which were commonly used in his era [68], [69]. He opened a door for new drug products by introducing sublimation and distillation in the preparation of medicines.
He described calcinations (roasting) of mercury and of arsenic in an oven to produce their oxides [70]. He prepared litharge (lead monoxide), white lead, lead sulphide (burnt lead), burnt copper, cadmia (calamine, which is native zinc carbonate), marcasite, yellow arsenic and lime, and numerous vitriols and salts [58], [65], [71]. He listed drug names and synonyms, with details of their stability, in Arabic, Greek, Syriac, Persian, and the vulgar tongue (Spanish) [68], [70].
Lady Isabel Burton stated that “anesthetics have been used in surgery throughout the East for centuries before ether and chloroform became the fashion in the civilized West” [72]. Indians used hyoscamus (henbane) and cannabis indica as anesthetics (Arabic: moukhadder) [73]. Arabs and Muslims used anesthetics to control pain during surgery by soporific (anesthetic) sponge [74]–[76]. Opium infusion was used commonly with painful procedures such as tooth removal and fracture reduction. Poppy seeds were used in oral analgesic syrups or paste. Muslims in Andalucía were the pioneers in using artificial ice-making for freezing the target place of patient’s body as a local anesthetic procedure [66].
Al-Zahrawi developed the anesthetic sponge (Arabic: al-esphanjah al-mourakkidah), which was the precursor of modern anesthesia. Before him, patients were given multiple doses of anesthetic solution during surgery. This predisposed the patients to the risk of overdose. Al- Zahrawi invented a sponge that was saturated with aromatics and soporifics and then dried. At the time for anesthesia, the sponge was immersed in a boiled solution and passed on the patient’s lips and nostrils. The boiled solution contained the active ingredients listed in Table 2. The ingredients were absorbed by the mucus membranes, causing deep sleep and pain control throughout the surgery. This type of anesthesia, “anesthesia by inhalation,” was known in Europe as “Arabian nights” [39], [46], [59], [61].
[accordion title=”Table 2. Natural Medicinal Products used in Anesthesia by Inhalation”]
| Common Name | Arabic Name | Effects |
|---|---|---|
| Hashih | Hasheesh | Mild euphoria |
| Opium | Afiun | Analgesic, narcotic |
| C-hyoscine | Cit al huscin | Gastrointestinal sedation, pain relief |
| Bearded darnel | Zoan | Dizziness, longer sleep |
[/accordion]
Although people of the era were unaware that bacteria causes sepsis, Al-Zahrawi used alcohol extracted from wine to keep his surgical instruments clean and to make spare tools ready for use in case of emergency [39], [59], [61].He used antiseptics in wounds and skin injuries [10], [13]. A powder consisting of incense, dragon’s blood, and quick or slaked lime was applied in the case of a small, uncomplicated wound. This powder has an antiseptic effect [77]. The giant ants used by Al-Zahrawi in surgical suturing secrete an antiseptic material (formic acid), which acts directly at the suture line [66].
Tar was used as antiseptic toothpaste. He used borax, which also has antiseptic properties and is a useful therapeutic for ulcers and throat infection. He used calcium carbonate contained in marble, nacre, or coral, which is still used as an antiseptic, tooth remineralizer, and teeth whitener. A mixture of verdigris and alum was applied to treat mouth chancre. Verdigris in combination with arsenic was a useful therapeutic for both bleeding and rotting gums [58]. He was a pioneer who used verdigris as a corrosive ointment to erode the remaining fat after a gynecomastia surgery. Also, verdigris has an anti-inflammatory effect [62], [63].
The Concealed Knife in General Surgery
![Figure 20: A concealed knife used in general surgery for incising abscesses [23]. (Photo courtesy of Fuat Sezgin.)](https://www.embs.org/wp-content/uploads/2016/03/retrospectroscope20-2516180.jpg)
Al-Zahrawi invented a concealed knife for incising abscesses, removing tumors and growths, and treating men struck by arrows. It resembles a kohl stick (kohl, usually antimony sulfide or lead sulfide, is used as eye makeup, especially in Eastern countries). The knife is made of copper and consists of a mobile lancet covered by an ellipsoid shell (secret chamber) attached to a handle, as shown in Figure 20. The lancet could be drawn out of the shell to the desired length and withdrawn again inside the shell. The knife is connected in that form to deceive the patient (especially a child) and not raise his or her anxiety, and that is clear from its name in Arabic, mokhdeaa, which means “the deceiver.” Also, this connection serves as a safety procedure for surgeons, decreasing the risk of cutting their own hands [11], [17], [21], [50], [79].
Conclusions
This article was meant to partially fill in one of the gaps in biomedical engineering history. Al-Zahrawi represents an important link in the chain of biomedical engineering history. The answer to the question “Could Al-Zahrawi be considered a biomedical engineer?” is certainly “yes.” Al-Zahrawi’s contributions involve a variety of biomedical engineering fields. His surgical instruments represent the biomechanics field. He invented a straight catheter as a treatment device. He used a metal probe as a diagnostic tool. The use of catgut in surgical suturing is an example of his contributions in the biomaterials field. He used ox bones as artificial teeth. The use of plaster in shoulder dislocation is an orthotic example in rehabilitation engineering. The fabrication of tablets represents his contribution in the chemical engineering field. He used the simulation concept in medical problems as he performed a tonsillectomy, tracheotomy, and craniotomy on a dead fetus. He represents a special model for the interaction between the biomedical engineer and the physician in the same person. Biomedical engineering students should know Al- Zahrawi for his numerous contributions to the field.
References
- J. D. Bronzino, “Biomedical engineering: a historical perspective,” in Introduction to Biomedical Engineering, J. D. Enderle and J. D. Bronzino, Eds. Amsterdam, The Netherlands: Elsevier/Academic Press, 2012, pp. 2–21.
- Z. O. Abu-Faraj, “Bioengineering/biomedical engineering education and career development: Literature review, definitions, and constructive recommendations,” Int. J. Eng. Educ., vol. 24, no. 5, pp. 990–1011, 2008.
- G. Gooday, J. M. Lynch, K. G. Wilson, and C. K. Barsky, “Does science education need the history of science?” Isis, vol. 99, no. 2, pp. 322–330, 2008.
- J. Requena-Carrion, R. S. Leder, M. Beebe, and M. Geselowitz, “The educational value of teaching biomedical engineering history,” in Proc. 32nd Annu. Int. Conf. IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 2010, pp. 316–318.
- A. Coppa, L. Bondioli, A. Cucina, D. W. Frayer, C. Jarrige, J.-F. Jarrige, G. Quivron, M. Rossi, M. Vidale, and R. Macchiarelli, “Palaeontology: Early Neolithic tradition of dentistry,” Nature, vol. 440, no. 7085, pp. 755–756, 2006.
- M. E. Valentinuzzi, “Why study the history of BME, science, and technology?,” IEEE Pulse, vol. 2, no. 1, pp. 45–47, 2011.
- M. Siebes, M. Viceconti, J. van der Sloten, N. Maglaveras, J. Kirkpatrick, and D. Kitney. (2005). Engineering for health: A partner in the development of a knowledge-based society for the benefit of European healthcare. [Online]. European Alliance of Medical and Biological Engineering and Science (EAMBES), Amsterdam, The Netherlands.
- M. C. Mendez and J. A. Leehan, “Overview of the biomedical engineering history in Mexico: A personal point of view,” in Proc. 25th Annu. Int. Conf. IEEE Engineering in Medicine and Biology Society (EMBS), Cancun, Mexico, 2003, pp. 3450–3453.
- F. Nebeker, “Golden accomplishments in biomedical engineering,” IEEE Eng. Med. Biol. Mag., vol. 21, no. 3, pp. 17–47, 2002.
- S. Kaf al-Ghazal. (2007). Al-Zahrawi (Albucasis) the great Andalusian surgeon. In Selected Gleanings from the History of Islamic Medicine. [Online]. M. El-Gomati, M. Abattouy, and S. Ayduz, Eds. Foundation for Science Technol & Civilization.
- C. A. Montagnani, “Pediatric surgery in Islamic medicine from the middle ages to the renaissance,” in Historical Aspects of Pediatric Surgery. Berlin, Heidelberg: Springer, 1986, pp. 39–51.
- F. S. Haddad, “Re endoscopic transvesical extramural ureterolithotomy,” Br. J. Urol., vol. 66, no. 6, pp. 668, 1990.
- S. Al-Benna, “Albucasis, a tenth-century scholar, physician and surgeon: His role in the history of plastic and reconstructive surgery,” Eur. J. Plast. Surg., vol. 35, no. 5, pp. 379–387, 2012.
- M. A. Elgohary, “Al Zahrawi: The father of modern surgery,” Ann. Pediatr. Surg., vol. 2, no. 2, pp. 82–87, 2006.
- M. K. Booz, “Albucasis bone surgery in antiquity,” Pan Arab J. Orthopaed. Trauma, vol. 1, no. 1, pp. 73–77, Nov. 1997.
- S. Amr and A. Tbakhi, “Abu Al Qasim Al Zahrawi (Albucasis): Pioneer of modern surgery,” Ann. Saudi Med., vol. 27, no. 3, pp. 220–221, 2007.
- E. Calvo, “Abu Al-Qasim Al-Zahrawi,” Aspetar Sports Med. J., vol. 1, no. 1, pp. 70–73, 2012.
- S. E. J. Golzari, Z. H. Khan, K. Ghabili, H. Hosseinzadeh, H. Soleimanpour, R. Azarfarin, A. Mahmoodpoor, S. Aslanabadi, and K. Ansarin, “Contributions of medieval Islamic physicians to the history of tracheostomy,” Anesth. Analges., vol. 116, no. 5, pp. 1123–1132, 2013.
- I. Masic, “The classics of Arabic medicine,” Med. Arch., vol. 64, no. 4, pp. 253–254, 2010.
- I. Hehmeyer and A. Khan, “Islam’s forgotten contributions to medical science,” Can. Med. Assoc. J., vol. 176, no. 10, pp. 1467–1468, May 2007.
- R. Hajar, “Al Zahrawi: Father of surgery,” Heart Views, vol. 7, no. 4, pp. 154–156, 2006.
- M. S. Spink, “Arabian gynaecological, obstetrical, and genito-urinary practice illustrated from Albucasis,” Proc. R. Soc. Med., vol. 30, no. 6, pp. 653–670, Apr. 1937.
- F. Sezgin and E. Neubauer, “Catalogue of the collection of instruments of the institute for the history of Arabic-Islamic sciences,” in Science and Technology in Islam, F. Sezgin, Ed. Frankfurt, Germany: Institut für Geschichte der Arabisch-Islamischen Wissenschaften an der Johann Wolfgang Goethe-Universität, 2010, pp. 36–91.
- C. J. S. Thompson, “The evolution and development of surgical instruments,” Br. J. Surg., vol. 26, no. 102, pp. 232–239, 1938.
- I. A. Nabri, “El Zahrawi (936-1013 AD), the father of operative surgery,” Ann. R. Coll. Surg. Engl., vol. 65, no. 2, pp. 132–134, Mar. 1983.
- I. Donaldson, “The cyrurgia of Albucasis and other works, 1500,” J. R. Coll. Physicians Edinb., vol. 41, no. 1, pp. 85–88, 2011.
- J. Kirkup, “The history and evolution of surgical instruments. VII. Spring forceps (tweezers), hooks and simple retractors,” Ann. R. Coll. Surg. Engl., vol. 78, no. 6, pp. 544–52, Nov. 1996.
- J. F. Lapena, “Mirrors and reflections: The evolution of indirect laryngoscopy,” Ann. Saudi Med., vol. 33, no. 2, pp. 177–181, Mar.–Apr. 2013.
- M. S. Spink and G. L. Lewis, Albucasis on Surgery and Instruments. A Definitive Edition of the Arabic Text with English Translation and Commentary. London, U.K.: Wellcome Institute of the History of Medicine, 1973.
- J. R. Kirkup, “The history and evolution of surgical instruments. I. Introduction,” Ann. R. Coll. Surg. Engl., vol. 63, no. 4, pp. 279–285, July 1981.
- R. E. Abdel-Halim, A. S. Altwaijiri, S. R. Elfaqih, and A. H. Mitwalli, “Extraction of urinary bladder stone as described by Abul-Qasim Khalaf Ibn Abbas Alzahrawi (Albucasis) (325-404 H, 930-1013 AD). A translation of original text and a commentary,” Saudi Med. J., vol. 24, no. 12, pp. 1283–1291, Dec. 2003.
- M. L. Al-Sudani, “5 Albucasis treatises in urology,” Eur. Urol. Suppl., vol. 8, no. 4, pp. 122, 2009.
- A. Tefekli and F. Cezayirli, “The history of urinary stones: In parallel with civilization,” Sci. World J., vol. 2013, no. 2013, 2013.
- M. E. Valentinuzzi, “The development of transfusion: Techniques and technology,” IEEE Pulse, vol. 2, no. 3, pp. 71–75, May/ June 2011.
- P. Missori, G. M. Brunetto, and M. Domenicucci, “Origin of the cannula for tracheotomy during the middle ages and Renaissance,” World J. Surg., vol. 36, no. 4, pp. 928–934, Apr. 2012.
- A. Aciduman and D. Belen, “Hydrocephalus and its management in Avicenna’s Canon of Medicine,” J. Neurosurg., vol. 106, no. 6 (Suppl), pp. 513–516, June 2007.
- M. Turgut, “Surgical scalpel used in the treatment of ‘infantile hydrocephalus’ by Al Zahrawi (936–1013 A.D.),” Child’s Nerv. Syst., vol. 25, no. 9, pp. 1043–1044, 2009.
- A. Aschoff, P. Kremer, B. Hashemi, and S. Kunze, “The scientific history of hydrocephalus and its treatment,” Neurosurg. Rev., vol. 22, pp. 67–93, 1999.
- N. R. F. Al-Rodhan and J. L. Fox, “Al-Zahrawi and Arabian neurosurgery, 936–1013 AD,” Surg. Neurol., vol. 26, no. 1, pp. 92–95, 1986.
- A. López-Valverde, N. López-Valverde- Hernández, M. Bravo, R. Gómez de Diego, E. Rosel, C. Gómez-Polo, G. Camañas, and J. Montero, “Dental practice in Al-Andalus (Spain) in the 10th and 11th centuries CE: Abulcasis Al-Zarahwi,” Int. J. Humanit. Soci. Sci. Educ. (IJHSSE), vol. 2, no. 3, pp. 64–70, Mar. 2015.
- S. Kaf al-Ghazal, “Al-Zahrawi (Albucasis): A light in the dark middle ages in Europe,” J. Int. Soc. Hist. Islam. Med. (JISHIM), vol. 1, no. 3, pp. 37–38, Apr. 2003.
- M. Romero and J. M. Saez, “Scope of Western surgical techniques to correct cleft lip and palate prior to the 18th century,” Cleft Palate Craniofac. J., vol. 51, no. 5, pp. 497–500, Sept. 2014.
- S. Nikhat and M. Fazil, “Kayi (cauterization): A tribute to Unani scholars,” Med. J. Islam. World Acad. Sci., vol. 21, no. 2, pp. 81–88, 2013.
- A. N. Kaadan and M. Angrini, “Who discovered hemophilia?” J. Int. Soc. Hist. Islam. Med. (JISHIM), vol. 8–9, no. 15–18, pp. 46–50, Apr./Oct. 2009–2010.
- L. F. Haas, “Albucasis or Abul Kasim (936–1013),” J. Neurol. Neurosurg. Psychiatr., vol. 54, no. 7, pp. 575, 1991.
- J. Annajjar, “Abu Alkasem AL Zehrawi (Albucasis 936-1013),” Child’s Nerv. Syst., vol. 26, no. 7, pp. 857–859, 2010.
- C. Singer, “The figures of the Bristol Guy de Chauliac M (circa 1430),” Proc. R. Soc. Med., vol. 10, no. Sect. Hist. Med., pp. 71– 90, 1917.
- S. Hamarneh, “Drawings and pharmacy in Al-Zahrawi’s 10th-century surgical treatise,” U.S. Natl. Museum Bull. 228, no. Paper 22, pp. 81–94, 1961.
- M. DeMaio, K. McHale, M. Lenhart, J. Garland, C. McIlvaine, and M. Rhode, “Plaster: Our orthopaedic heritage: AAOS exhibit selection,” J. Bone Joint Surg. Am., vol. 94, no. 20, pp. e152, Oct. 2012.
- E. Savaage-Smith, “The practice of surgery in Islamic lands: Myth and reality,” Soc. Hist. Med., vol. 13, no. 2, pp. 307–321, 2000.
- F. Dibsi, “Surgical diseases of the mouth and throat by Albucasis,” Int. Congr. Ser., vol. 1240, pp. 1375–1378, 2003.
- J. Kirkup, “The history and evolution of surgical instruments. III. Handles,” Ann. R. Coll. Surg. Engl., vol. 65, no. 4, pp. 269– 273, July 1983.
- J. B. Anderson and A. J. Webb, “Fine-needle aspiration biopsy and the diagnosis of thyroid cancer,” Br. J. Surg., vol. 74, no. 4, pp. 292–296, Apr. 1987.
- J. Kirkup, “Surgical history. The history and evolution of surgical instruments. VIII. Catheters, hollow needles and other tubular instruments,” Ann. R. Coll. Surg. Engl., vol. 80, no. 2, pp. 81–90, Mar. 1998.
- S. R. Yedke, S. Y. Raut, and C. R. Jangde, “Experimental evaluation of horse hair as a nonabsorbable monofilament suture,” J. Ayurveda Integr. Med., vol. 4, no. 4, pp. 206–210, Oct.–Dec. 2013.
- A. Zargaran, A. Mehdizadeh, and A. Mohagheghzadeh, “Brief report: Cataract surgery in Albucasis manuscript,” Iran. J. Ophthalmol., vol. 24, no. 1, pp. 75–76, 2012.
- J. A. Donaldson, “The use of gold in dentistry: An historical overview. Part I,” Gold Bull., vol. 13, no. 3, pp. 117–124, 1980.
- J. Carrasco and M. Liñán, “The stomatological use of stones cited in the Kitab al-tasrif treatise (Abulcasis, 1000 CE),” Geological Soc., London, Special Publ., vol. 375, no. 1, pp. 65–80, Jan. 2013.
- R. Moreno-Otero, “Abulcasis, the father of modern surgery,” Med. Arch., vol. 67, no. 2, pp. 151, 2013.
- A. M. K. Sherwani, A. N. Ansari, H. A. H. Ansari, and I. A. J. A. Ansari, “The contribution of Albucasis (Abul-Qasim Zahravi) in venesection,” J. Int. Soc. Hist. Islam. Med. (JISHIM), vol. 3, no. 5, pp. 6–8, Apr. 2004.
- J. Najjar, “From anesthetic sponge to nonsinking skull perforator, unitary work neurosurgery in the ancient Arabic and Islamic world,” World Neurosurg., vol. 73, no. 5, pp. 587–594, 2010.
- A. N. Kaadan and H. Khawatmi. The drugs which Zahrawi used in surgical medicine. [Online]. Int. Soc. Hist. Islam. Med. (ISHIM).
- S. H. Chavoushi, K. Ghabili, A. Kazemi, A. Aslanabadi, S. Babapour, R. Ahmedli, and S. E. Golzari, “Surgery for gynecomastia in the Islamic golden age: Al-Tasrif of Al-Zahrawi (936-1013 AD),” ISRN Surg., vol. 2012, no. 2012, 2012.
- P. M. Dewick, Medicinal Natural Products, 3rd ed. Hoboken, NJ: Wiley, 2009.
- S. T. S. Al-Hassani, E. Woodcock, and R. Saoud, 1001 Inventions: Muslim Heritage in Our World, 2nd ed. U.K.: Foundation for Science Technology and Civilization, 2007.
- M. A. Fallouji, “History of surgery of the abdominal cavity. Arabic contributions,” Int. Surg., vol. 78, no. 3, pp. 236–238, July–Sept. 1993.
- S. K. Hamarneh, “The first known independent treatise on cosmetology in Spain,” Bull. Hist. Med., vol. 39, no. 4, pp. 309–325, July–Aug. 1965.
- S. K. Hamarneh and G. A. Sonnedecker, “General survey of the content and structure of al-Tasrif,” in A Pharmaceutical View of Abulcasis Al-Zahra¯wı¯ in Moorish Spain: with Special Reference to the “Adha¯n.” Leiden, The Netherlands: E. J. Brill, 1963, pp. 65–74.
- S. Anjum, “Al-Zahrawi: A prominent Muslim medical scientist and his impact on West,” Revelat. Sci., vol. 3, no. 2, pp. 51–56, 2013.
- W. Sneader, “The Arab world,” in Drug Discovery: A History. West Sussex, U.K.: Wiley, 2005, pp. 26–29.
- E. Ravina, “Evolution of drug discovery,” in The Evolution of Drug Discovery: From Traditional Medicines to Modern Drugs, E. Ravina and H. Kubinyi, Eds. Weinheim, Germany: Wiley, 2011, p. 6.
- L. I. Burton, “1001 nights,” in The Book of the Thousand Nights and One Night, R. F. Burton, Ed. London, U.K.: Modern Press Library, 1886, pp. 1885–1888.
- M. S. M. Takrouri, “Historical essay: An Arabic surgeon, Ibn al Quff’s (1232–1286) account on surgical pain relief,” Anesth., Essays Research., vol. 4, no. 1, pp. 4–8, Jan.–June 2010.
- J. Keller, “An exploration of anaesthesia through antiquity,” Univ. West. Ontario Med. J. (UWOMJ), vol. 78, no. 1, pp. 49–52, 2008.
- P. Prioreschi, “Medieval anesthesia—the spongia somnifera,” Med. Hypotheses, vol. 61, no. 2, pp. 213–219, Aug. 2003.
- A. M. Bhat, “Anesthesia drugs in the medieval Muslim era,” Int. J. Sci. Eng. Res., vol. 4, no. 3, pp. 1–9, Mar. 2013.
- Z. Cope, “The treatment of wounds through the ages,” Med. Hist., vol. 2, no. 3, pp. 163–174, July 1958.
- J. M. Taha, “Unknown contributions of the Arab and Islamic medicine in the field of anaesthesia in the West,” J. Int. Soc. Hist. Islam. Med. (JISHIM), vol. 6–7, no. 11–14, pp. 67–71, Apr./Oct. 2007–2008.
- S. A. Ahmadi, A. Zargaran, A. Mehdizadeh, and M. J. Mortazavi, “Remanufacturing and evaluation of Al Zahrawi’s surgical instruments, Al Mokhdea as scalpel handle,” Galen Med. J., vol. 2, no. 1, pp. 22–25, 2013