[accordion title=”Introducing the Authors”]
When the stream is driven by a powerful pump, the running waters can take you to the unknowns of the mind.
—Max E. Valentinuzzi
Elisa Pérez was born in San Juan, Argentina, in 1978. She graduated as a bioengineer from the Universidad Nacional de San Juan (UNSJ) in 2004 and later obtained a doctorate in control systems, also at UNSJ, in 2010. Currently, she is an associate professor with the Gabinete de Tecnología Médica (GATEME-UNSJ) and is assistant investigator at Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET). Her research interests are image processing, human–computer interfaces, and control of robotic wheelchairs. Elisa had considerable sweat and tears come out of her eyes while trying to solve the many difficulties that day by day popped up from the darkness.
Sergio D. Ponce obtained an electronics engineering degree from the Universidad Tecnológica Nacional (UTN), San Nicolás, in 2000, with several graduate courses taken at the Universidad Favaloro in Buenos Aires City, and a degree in technological management from UTN. He is a professor of applied electronics and, since 2006, also a coordinator of the Clinical Engineering Program at UTN and secretary to the Municipal Agency of Science and Technology of San Nicolás. His research interests include signal processing, electromedical equipment design, bioinformatics, and management of medical technologies. Sergio inserted a critical eye into the project from which several significant changes were introduced.
David J. Piccinini is the youngest member of the team. David is a native of Villa Unión, Province of Santa Fe, the place where he saw, for the first time, the sunlight in 1991. He received a technical degree in electronics from a second-level school. He is now an advanced student of electronics engineering at UTN, San Nicolás, under a fellowship supported by the Grupo de Análisis, Desarrollos e Investigaciones Biomédicas of the same institution. He is attracted to programming the so-called embedded systems, that is, computer systems with a dedicated function within a larger mechanical or electrical system. Simultaneously, he likes to search into the social meanings of such innovative developments. In many respects, he was a kind of worker bee quietly carrying out the many tasks the bigger guys asked him to do, tasks not to be neglected or looked down upon but quite necessary, indeed.
The powerful pump is represented by Natalia López (pure sanjuaninobred and born in 1975), a young biomedical engineer with a bachelor’s degree in bioengineering and master’s and doctorate degrees in control engineering from UNSJ, in 2001, 2007, and 2010, respectively. In 2003, she joined GATEME-UNSJ, where she is currently an associate professor while holding the position of assistant investigator at CONICET. Her research is focused on biomedical signal processing, especially electromyographic signals, assistive devices, and the application of robotics in stroke and upper-limb rehabilitation. By “powerful pump,” I mean she has been instrumental in pushing this project forward, be it at UNSJ or at San Nicolás, a nice town in the northern area of the Province of Buenos Aires, rather close to the Santa Fe province.
Finally, to close this introduction—I do not quite understand, but this group of authors insisted in adding my worn out (but not yet rusty) name in the byline of this article. This is perhaps a kind and, to me, a highly appreciated gesture. I merely dug into the historical development of the subject, did some writing, and learned a lot, while new information keeps appearing, such as the book by Dr. Dorita S. Berger, Eurhythmics for Autism and other Neurophysiologic Diagnoses (Jessica Kingsley Publishers, London), with a foreword by Dr. Stephen M. Shore.
—Max E. Valentinuzzi
[/accordion]
Mind and consciousness are like a gradual sunrise that takes time to come up. In the meantime, we are not stagnant, waiting for life to happen. The music of life, felt with our bodies, long before we identify mind with self…some of us stay here longer than others. Music in its broader sense is everywhere, and it is our first language…it has the most important of all places in the lives of those who find the realm of the mind a place of rusty cogs and heavy effort.
—Donna Williams, (from the preface of [11], with a review by Max E. Valentinuzzi in [12])
One symptom common to all types of autism is an inability to easily communicate and interact with others. In fact, some people with autism are unable to communicate at all. Others may have difficulty interpreting body language or holding a conversation.
The Swiss physician Paul Eugen Bleuler (1857–1939) coined the term autism in 1908 when describing a schizophrenic patient who had withdrawn into his own world. Bleuler actually used it to mean “morbid self-admiration” and some kind of inner hiding. Later, an Austrian pediatrician, Hans Asperger (1906–1980), studied mental disorders in children. His work only acquired world renown posthumously. A resurgence of interest in his work began in the 1980s, in particular, because of the pediatric diagnosis of autistic psychopathy and what is now called Asperger’s syndrome, a specific autism that is characterized by significant difficulties in social interaction and nonverbal communication.
Leo Kanner (1894–1981) was an Austrian-American psychiatrist also known for his work related to autism; he organized the foundation of child and adolescent psychiatry in the United States and worldwide. Kanner was born in Klekotow, a small village in what is now considered the Ukranian jurisdiction. He studied at the University of Berlin, receiving his M.D. degree in 1921 and immigrating to the United States in 1924. In 1930, he was selected to develop the first child psychiatry service at Johns Hopkins Hospital in Baltimore, Maryland. His 1943 paper, “Autistic Disturbances of Affective Contact,” along with the work of Hans Asperger, forms the basis of the modern study of autism. Thus, autism as such is barely more than 100 years old.
The objectives of this article are twofold: first, to briefly review the relatively short history of the condition and, second, to introduce a graphical user interface especially designed for children with autism spectrum disorder (ASD). We also address the efforts currently being made with music therapy.
A Few More Historical Hallmarks
In September 2013, the American Psychiatric Association released the fifth edition of its Diagnostic and Statistical Manual of Mental Disorders, often referred to as DSM-5, and The New England Journal of Medicine featured a historical perspective on autism to mark the 70th anniversary of Leo Kanner’s momentous description of the disorder in 1943. The 1943 paper described 11 children who shared the qualities of high intelligence, a profound preference for being alone, and an obsessive insistence on the preservation of sameness. The children had difficulties in social interactions, difficulty in adapting to changes in routines, good memory, sensitivity to stimuli (especially sound—a good point to underline in light of some positive reported results with music therapy), resistance and/or allergies to certain foods, good intellectual potential, echolalia or propensity to repeat words or sounds they hear, and difficulties in spontaneous activity.
The 1970s brought an understanding that autism stemmed from biological differences in brain development. Objective criteria for diagnosing autism followed in the 1980s, and so did a clear separation from childhood schizophrenia. Note how recently these developments were made: just about 35 years ago. During the 1950s and 1960s, mothers were blamed by psychoanalysts, with some being called “cold moms.” In 1987, DSM laid out a checklist of criteria for the diagnosis of autism, and between 1994 and 2000, the definition was expanded to include Asperger’s syndrome. Hans Asperger’s patients in 1944 resembled Kanner’s earlier descriptions, but the children Asperger studied did not have echolalia as a linguistic problem; they spoke like adults. He also mentioned that many of the children were clumsy and different from normal children in terms of fine motor skills. Very recently, as of 2013, DSM folded all subcategories under one umbrella: ASD. It is defined by two categories: impaired social communication and/or interaction and restricted and/or repetitive behaviors.
There are other names within the field of autism research that should be mentioned, with conflicting opinions and also with agreements, but all produced significant knowledge.
- Bruno Bettelheim (1903–1990), an Austrian-born psychoanalyst and survivor of the Dachau and Buchenwald Nazi concentration camps, settled in the United States in 1939. At the University of Chicago, in Illinois, he carried out studies based on clinical practice. After suffering a stroke and deep depression due to his wife’s death, he unfortunately committed suicide.
- Bernard Rimland (1928–2006) was an American psychologist and a parent of a child with autism. He disagreed with Bettelheim’s ideas. His research led him to believe that autism is a biological disorder, not one of the mind, and certainly not the mother’s fault. In 1965, Rimland founded the National Society for Autistic Children (now the Autism Society of America) to promote a highly controversial behavioral modification therapy developed by Ivar Lovass (see below); that therapy is known today as applied behavioral analysis. Rimland also investigated the use of high doses of vitamin B6, which appeared preposterous at first but has since been proven beneficial. In 1967, he founded the Autism Research Institute.
- Lorna Wing (1928–2014) was an English physician who contributed in the field of childhood developmental disorders. She introduced the term Asperger’s syndrome and was involved in founding the U.K. National Autistic Society.
- Lars Christopher Gillberg (1950–present) is a professor of child and adolescent psychiatry at Gothenburg University, Sweden. Gillberg’s extensive research has significantly advanced the field of child and adolescent neuropsychiatry in areas such as ASD, epilepsy, intellectual disability, oppositional defiant disorder, Tourette’s syndrome, and anorexia nervosa.
- Lars Christopher Gillberg (1950–present) is a professor of child and adolescent psychiatry at Gothenburg University, Sweden. Gillberg’s extensive research has significantly advanced the field of child and adolescent neuropsychiatry in areas such as ASD, epilepsy, intellectual disability, oppositional defiant disorder, Tourette’s syndrome, and anorexia nervosa.
- Ole Ivar Lovaas (1927–2010), born in Norway, studied and furthered behavioral analysis and treatment of children with autism. He was a clinical psychologist at the University of California at Los Angeles and pioneered a treatment for autism known today as the Lovaas treatment.
It must be underlined that in the 1960s–1970s, research into treatments for autism focused on medications such as lysergic acid diethylamide, electric shock, and behavioral-change techniques. It is difficult to believe, but the latter relied on pain and punishment. Fortunately, during the 1980s and 1990s, the role of behavioral therapy and the use of highly controlled learning environments emerged as the primary treatments for many forms of autism and related conditions. Currently, the cornerstones of autism therapy are behavioral therapy and language therapy. Surprisingly, music and bioengineering were rarely (if ever) mentioned as possible helpful resources.
As of 2010, the rate of autism was estimated at about one to two per 1,000 people worldwide, and it occurs four to five times more often in boys than girls. About 1.5% of children in the United States (one in 68) were diagnosed with ASD as of 2014, a 30% increase from one in 88 in 2012. The rate of autism among adults aged 18 years and over in the United Kingdom is 1.1% [1], [2]. The question of whether actual rates have increased is unresolved and is obviously an open area of research where biomedical engineering can help. Early detection is very important for a correct approach to treatment and stimulation in children, improving the likelihood of success for the adaptive, cognitive, and linguistic processes.
BME Interfaces
Whoever thought of an engineer trying to fix a child’s complex and delicate mind? But why not? An interface—designed to be simple, easy to manage, and friendly, with activities that stimulate cognitive and motor growth—was created to bring the autistic child out of his or her hiding place, or, at least, to partially assist him or her in such an opening maneuver. A performance index and system usability scale (SUS) were used to evaluate the performance of the children when they used the interface. The evaluation was carried out with a group of children that suffer from ASD and who regularly attended phonoaudiology therapy at a state hospital. The results were very encouraging because the children showed interest in using the software. Besides, the quantitative evaluation proved that the graphic interface is simpler to use than the conventional environment.
Background
Although the involvement of bioengineering in the subject is not totally new, it can be stated that it is rather recent, as attested by a few publications. A Portuguese group in Lisbon presented a multimedia platform to overcome ASD children’s communication and social difficulties. Their results showed that children felt motivated after using the tool, and the number of interactions between peers increased. Their platform can be customized, and the authors introduced an evaluation methodology [3].
Around the same time as the authors of [3], a Greek research group from the University of Ioannina reported an application within the widely emergent area of information and communication technologies [4]. They stated that the diversity of characteristics encountered by children with learning and communication difficulties may present an extra challenge for potential hypermedia application developers. The ultimate goal of such exercises is to facilitate the learning environments of the target population. Six cases with mental retardation and autism have been taught using their application. All of the children showed significant progress after instruction on the specific components. The required number of sessions for all children varied according to their ability level and severity of their needs. Overall, it seems that the application has the potential to help children learn the concepts it addresses.
In a Canadian pilot project, Michelle Wang and Denise Reid studied the efficacy of a novel virtual-reality cognitive rehabilitation intervention to improve contextual processing of objects in children with autism. They tested four children with autism in a multiple-baseline, single-subject study. The children were taught how to see objects in context by reinforcing attention to pivotal contextual information. All children demonstrated statistically significant improvements in contextual processing and cognitive flexibility. Mixed results were found on the control test and changes in context-related behaviors. It was concluded that larger-scale studies are warranted to determine the effectiveness and usability in comprehensive educational programs [5].
Mintz, in turn, in 2013, reported a qualitative evaluation of a special project prototype, identifying which factors mediate the level of engagement with technology by both teachers and children with ASD. This project developed a mobile cognitive support application for smartphones, based on the principles of persuasive technology design [6].
Sue Fletcher-Watson, of the University of Edinburgh, United Kingdom, says, in a well-referenced and updated review, that computer-assisted learning (CAL) is an approach that has been widely used to support people with ASD. Commercial and research-driven technologies continue to be produced at a rapid rate, particularly mobile device applications. However, the field lacks a consistent, evidence-based methodology for design, implementation, and evaluation of these technologies. The review collates published evidence for the value of CAL in autism education and therapy, with a specific view to identifying best practices in design, implementation, and evaluation. The future of research in CAL for autism is considered, including the need for relevant theoretical underpinnings and appropriate responses from researchers and practitioners to novel technologies [7].
What News We May Suggest: A Practical Example
This section describes the experience obtained at a public hospital following requirements outlined by the attending physicians to a group of children with different ASD degrees, that is, by using a friendly software environment with activities aimed at improving the communication and the interaction of the children with the computer. The proposed interface is an assistive technology, and, as such, it was defined as a human activity assistive technology model for the purpose of its evaluation [8]. This model considers that the assistive system is composed of
- the user (a person with a disability)
- the activity (a task carried out by the user)
- the assistive technology (a device to carry out the activity)
- context (the environment where the user performs the task).
The system was evaluated as a whole using different parameters, such as the throughput (TP) performance index for each user (which is based on Fitts’s law to compare the users’ performances in specific tasks). Fitts’s law is a descriptive model of human movement primarily used in human–computer interaction and ergonomics. It predicts that the time required to rapidly move to a target area is a function of the ratio between the distance to the target and the width of the target. Paul Fitts also proposed an index of performance (IP), measured in bits per second, as a measure of human performance—i.e., the average rate of information generated by a series of movements is the average information per movement divided by the time per movement. Nowadays, IP is more commonly called TP, i.e., it is the amount of work that a computer can do in a given time period [9].
Each user responded to a poll based on the SUS to obtain his or her opinion on the interface. In this way, the system was tested with eight children with ASD, and the data obtained in the experiments provided a quantitative evaluation of the system and a performance evaluation of the children [10].
Software Design and Development
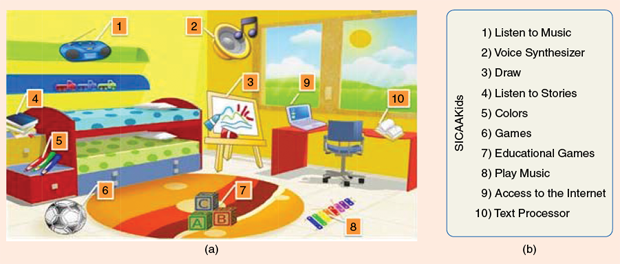
The platform designed works under any operating system. It was programmed with Microsoft Visual Basic.Net 2008 Express, which is free, provided by Microsoft Corporation on its website. The design is simple and attractive, with pictures that relate the icons with the underlying functions. The scenario chosen is a child’s room (Figure 1). Since many of the children are not literate, the platform is based on images and their association possibilities. The name of the interface is SICAAKids (in Spanish, Sistema Integrado de Comunicación y Asistencia Automatizada, or Automatized Integrated Communication and Assistive System Intended for Kids). All the embedded programs (music, educational games, and others) are public license. These functions were implemented in accordance with the activities that phonoaudiologists carry out at the hospital.
The available functions are as follows:
- Listen to music: Music is of paramount importance in the intellectual, auditory, sensory, speech, and motor development of the child. The child is capable of expressing himself or herself differently as well as integrating actively into society; music helps him or her achieve autonomy in daily activities, take care of himself or herself, be more aware of his or her surroundings, and widen relationships (see, e.g., Donna Williams’ words at the beginning of this article).
- Voice synthesizer: Icons that have activities and feelings are displayed so that the child selects the icon he or she wants to explore.
- Draw: Drawing can have a clear intention of communication, showing characters and emotions.
- Listen to stories: Reading stories to children helps them stimulate their speech and imagination. Often, ASD children are not incentivized enough in this respect. In addition, stories can have a relaxing effect. In this activity, there is an option to record the stories with the parents’ voices and add new stories, given that these children prefer to listen to familiar voices, and other sounds or noises tend to disturb them.
- Colors: Colors are visual stimuli that can generate reactions in the body and in mood, too. In addition, they help memorization.
- Games: Play is the natural activity that children use to adapt to life, to learn, to have fun, and to relate to others. It is such a basic necessity in childhood that the old Summerhill School in England (founded by Alexander S. Neill in 1921) used to be quite open, giving its pupils total freedom. Games have a decisive role in the child’s development because it allows him or her not only to enjoy but also to manifest happiness, fears, anxieties, and needs.
- Educational games: It is effective to associate animals with the sounds they produce, which is quite important in language development. Memory games also speed up information retention.
- Play music: Acting as powerful central nervous system stimulation, music helps the child in his or her creative abilities.
- Access to the Internet: This function connects the child with other environments and, hence, gives him or her a sense of socializing.
- Text processor: It orients the child to work with other children when reading and writing.
Assistive Technology Evaluation and Tests
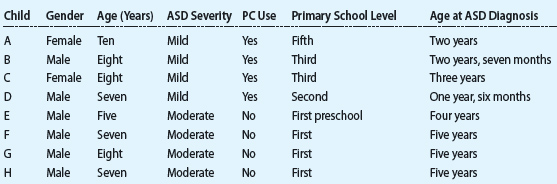
Both system and user performance are involved when the user carries out an activity using assistive technology. The human performance can be defined as the result of a set of actions tending to satisfy an objective, by and large, according to some standard. By the same token, the assistive technology is the more or less effective tool employed by the operator. The proposed interface was implemented and evaluated with eight ASD children. Tests were carried out in three different sessions after their parents signed the informed consent form. The children were selected according to the following criteria:
- a diagnosis of ASD by a pediatric neurologist
- a chronological age between four and ten years
- a mild to moderate ASD diagnosis (Table 1).
Table 1: Groups and Characteristics for Children with ASD.
The activity consisted of moving the cursor on the screen 15 times to different icons. The cursor had to be moved 15 times, that is, there were 15 repetitions. Fitts’s law predicts the time taken for a human movement from pointing an initial object i to a final object f. The law is expressed as a linear function of the distance between the object and the wide dimension of the final object, i.e., as (1) describes. Besides, it assumed that the participant makes the movement as fast as possible.
MT = a + b * ID, (1)
where MT stands for movement time, ID is the difficulty index, a represents the Y-intercept, and b is the straight-line slope. The values of a and b were calculated by least square regression. The difficulty index is defined as
![]()
where D, expressed in bits, is the distance from the initial position to the end point, and W stands for the width of the selected object. Since the purpose of the analysis is to compare two or more different conditions of the same experiment, the TP value is obtained as
![]()
where IDe is the mean value of the measurements. It can be noted from (3) that a value of TP is first obtained for each subject (as a mean performance achieved by the subject over all x movement conditions), and then these TP values are averaged to obtain the final TP index (y represents the number of subjects). When TP is calculated as previously explained, it represents a complete measure that includes information about both the speed and accuracy of the movement performance. Speed and accuracy are averaged, and, therefore, they combine the effects of the slope and intercept parameters into one measure that can be compared between conditions and studies. All tests were run in an isolated room and implemented with a computer where the software was installed.
Usability, defined as the effectiveness, efficiency, and satisfaction, by which users achieve their goals in different contexts, was also quantified by means of the SUS scale (see [10]). It is a simple scale of ten items that provides a global vision of the subjective evaluations. Each question is graded from 1 to 5 (1 = absolute disagreement; 5 = full agreement), and all partial results must be added up. Scores were calculated following the procedure given by Brooks in 1996 [10].
The following ten simplified items were presented to the children:
- I think I would like to use this program every time I can.
- I found the program unnecessarily difficult.
- I thought the program would be easier to use.
- I think I would need the phonoaudiologist’s help to use the program.
- I easily found the different icons of the program.
- I did not understand the program.
- I imagine that most people would learn to use the program fast.
- I found the program too long to go through.
- I felt very confident to manage the program.
- I need to learn many things before I can manage the program.
The children were divided in two groups (Table 1, above). The first group comprised children with mild ASD (subjects A–D). They go to school and are integrated in different schools. This group included one ten-year-old (subject A), two eight-year-olds (subjects B and C), and one seven-year- old (subject D). All of them were familiar with computers, and the use of the computers was according to their ages. The second group (subjects E–H) included one five-year-old (subject E), two seven-year-olds (subjects F and H), and one eight-year-old (subject G). Each test was carried out in two phases: one with a Windows desktop and the other with SICAAKids. The TP was calculated for each selected icon, both in the SICAAKids software and in Windows. The MT defined in (1) was calculated by software for each user.
What Was Obtained
SICAAKids
The SICAAKids icons were a computer, which stands for Internet access (TPS1); pencils, whose function is painting (TPS2); and cubes, which represent games (TPS3).
Desktop Environment
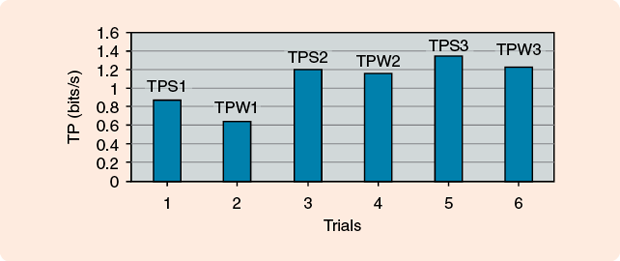
Three Windows access icons, INTERNET (TPW1), PAINT (TPW2), and GAMES (TPW3), were placed on the computer desktop, located at the same distance that they appear on the SICAAKids screen. Their sizes were enlarged with the Windows accessibility tools so that the icons’ widths were comparable. The time that the user took to go from the right top margin to the corresponding icon was evaluated 15 times for each icon. For comparison between WINDOWS and SICAAKids, three icons were chosen from the former such that they represented the same activities of the latter. They were named, respectively, INTERNET (TPW1), PAINT (TPW2), and GAMES (TPW3).
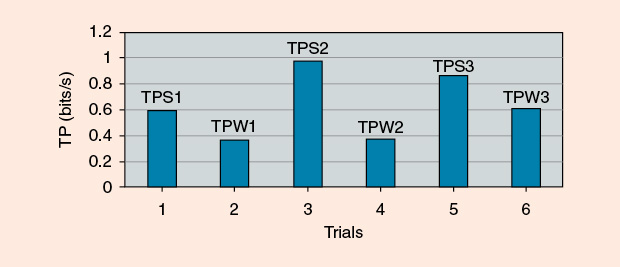
Figure 2 compares trials among the TPs of the first group. As can be observed, all TP values related to SICCAKids are larger than the ones obtained with Windows. This represents a positive evaluation of the proposed system; children who are used to Windows got a better TP with SICCAKids. Figure 3 shows the TPs that were obtained with the second group. The values are lower than for group 1; however, with SICCAKids, the scores are still better than with the Windows desktop. It must be remarked that group 2 was difficult to evaluate because the children were not interested in the Windows desktop. The values obtained in the scale are quite high, with an average above 80 (Table 2).
Table 2: SUS Values
| Subject | SUS Value |
| A | 97 |
| B | 90 |
| C | 92 |
| D | 90 |
| E | 60 |
| F | 87 |
| G | 80 |
| H | 78 |
| Total Average | 84.25 |
Discussion
There are several aspects in this not common but emotionally touching behavioral problem that need to be underlined. First, its identification and correct recognition are rather recent, and, in some aspects, so much so that the intended therapies were not only absolutely wrong but cruel. Second, it must be accepted that autism projects itself beyond the medical environment, having become a true interdisciplinary condition that calls for different inputs, and engineering and biomedical engineering appear as new areas with a wide spectrum of resources. A very recent IEEE Institute Alert newsletter [13] (regarding the Consumer Electronics Show) explores new applications designed to benefit humanity and even save lives [10]. It reports on a recent system to encourage children with autism to participate in imaginative play.
Regarding the system described here, we must admit that, even though the results are encouraging, the sample was small, and further and larger tests are needed. Also, the groups should be divided according to the level of the children’s familiarity with technology. Parents should take home the software and make it a daily activity, for real play, similar to taking the child to a playground. Another possibility would be to make the software compatible with Android, which is an operating system that usually runs on smartphones and tablets. Since it is an opensource operating system, users can adapt it and run it on a personal computer. Linguistic elements could also be incorporated and help with the phonoaudiology therapy.
It should be mentioned that the use of music as a tool to rehabilitate autistic children is an area where there is ample experience, although quantitative results are not easy to give because no evaluation procedure has been developed yet, except of the qualitative type. References [11] and [12], mentioned at the beginning of this article, can be used as guide. Dorita Berger is a dedicated and a long-time music therapist and concert pianist. There is more information regarding this aspect on the web.
Conclusions
A historical review of autism was presented, showing that, only recently, have better and proper steps been taken for its treatment, including elements obtained from other disciplines that were previously unthinkable. New software for children with ASD has been developed. The system is simple, friendly, and obtained good acceptance from children while also arousing their interest. These characteristics favorably affected the children’s response, and the scores tend to back this up.
Acknowledgments
All tests were carried out at the Guillermo Rawson Hospital (the main provincial hospital in San Juan City, Argentina), where kind assistance was provided by the medical and paramedical personnel.
References
- Centers for Disease Control and Prevention Office of Surveillance, Epidemiology, and Laboratory Services, “Prevalence of autism spectrum disorders—Autism and developmental disabilities monitoring network, 14 Sites, United States, 2008,” Morbidity Mortality Weekly Rep., U.S. Dept. Health and Human Services, Atlanta, GA; Surveillance Summaries, Mar. 30, vol. 61, no. 3, 2012.
- R. P. Seldas. (2012). Los síntomas de los trastornos del espectro de autismo en los primeros dos años de vida: Una revisión a partir de estudios longitudinales prospectivos (in Spanish, Symptoms of the ASD in the first two years of life: A review starting with longitudinal prospective studies). [Online]. Anales de Pediatría (Barcelona, Spain), 76(1), e1–41.e10.
- M. L. da Silva, D. Gonçalves, T. Guerreiro, and H. Silva, “A web-based application to address individual interests of children with autism spectrum disorders (ASD),” Procedia Comput. Sci., vol. 14, pp. 20–27, 2012.
- E. Morfidi, T. Mikropoulos, and I. Bellou, “Teaching intervention through a hypermedia application for children with learning and communication difficulties,” Procedia Comput. Sci., vol. 14, pp. 419–427, 2012.
- M. Wang and D. Reid. (2013, Nov. 13). Using the virtual reality-cognitive rehabilitation approach to improve contextual processing in children with autism. [Online]. Sci. World J., 2013, 9.
- J. Mintz. (2013). Additional key factors mediating the use of a mobile technology tool designed to develop social and life skills in children with autism spectrum disorders: Evaluation of the 2nd HANDS prototype. [Online]. Comput. Educ., 63, 17–27.
- S. Fletcher-Watson, “A targeted review of computer-assisted learning (CAL) for people with Autism Spectrum Disorder (ASD): Towards a consistent methodology,” J. Autism Develop. Disorders, vol. 1, no. 2, pp. 87–100, 2014.
- A. M. Cook and J. M. Polgar, Assistive Technologies: Principles and Practice. Mosby, Saint Louis, MO: Elsevier Health Sciences, 2014.
- P. M. Fitts, “The information capacity of the human motor system in controlling the amplitude of movement,” J. Exp. Psychol., vol. 47, no. 6, pp. 381– 391, 1954.
- J. Brooke, “SUS: A ‘quick and dirty’ usability scale,” in Usability Evaluation in Industry, P. W. Jordan, B. Thomas, B. A. Weerdmeester, and A. L. McClelland, Eds. London, U.K.: Taylor & Francis, 1996, pp. 189–194.
- D. S. Berger, Music Therapy, Sensory Integration and the Autistic Child. London, U.K.: Jessica Kingsley Publ. Ltd., 2002.
- M. E. Valentinuzzi, “Review of ‘Therapy, sensory integration and the autistic child’ by DS. Berger,“ BioMed. Eng. On-Line, vol. 4, no. 9, Feb. 2005.
- L. Nachman, “Leveraging technology to help people with disabilities,” IEEE Institute Alert, Apr. 2015