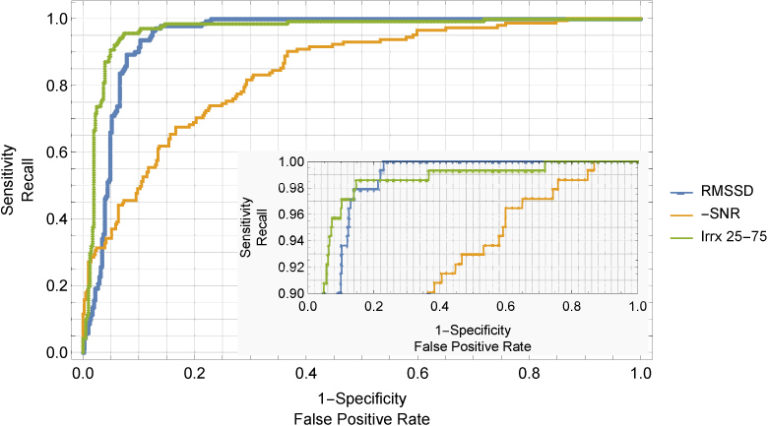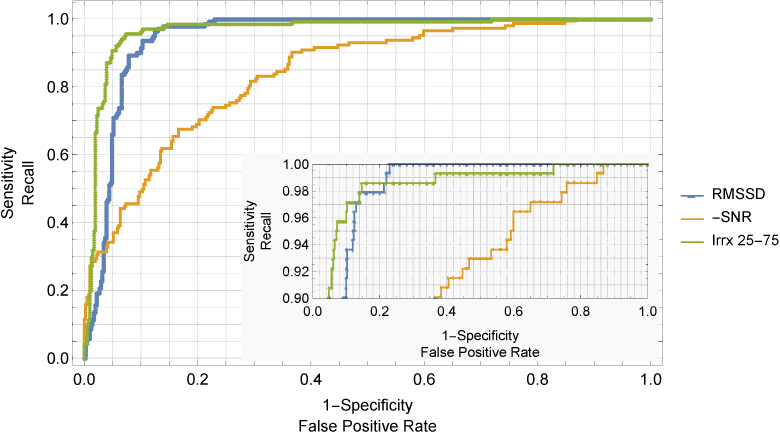
Atrial fibrillation (Afib) contributes significantly to overall cardiovascular risk. Widespread screening for Afib in primary care is sometimes performed by palpation, but suffers from low accuracy and is dependent on clinician experience. Algorithms implemented on oscillometric blood pressure devices can detect Afib with high sensitivity and specificity, but information on factors affecting accuracy is scant. Concurrent diagnostic electrocardiogram (ECG) and oscillometry were measured in participants in ECG clinics at two sites. Root mean squared successive difference (RMSSD) and irregularity index (Irrx) were calculated from oscillometric data and used to train logistic regression classifiers. Monte Carlo cross validation with 20 splits was performed to estimate confidence intervals for mean sensitivity and specificity, with various weightings, in the absence or presence of ectopics, and with or without repeated measurements. 707 measurements, including 168 Afib, were collected from 569 participants with mean (standard deviation) age of 63 (16) years. Sensitivity/specificity of RMSSD and Irrx were 0.982/0.908 and 0.986/0.960 respectively when ectopics were included. Excluding ectopics from the data improved specificity by up to 5%. Nevertheless, based on this performance and after accounting for prevalence of Afib in the population aged over 60 years, and estimated costs of healthcare, oscillometric screening for Afib in this age group could return a positive net health-economic benefit.