
Medical students are attracted by the prospect of a meaningful addition to their clinical work. Engineering students are excited by a unique opportunity to learn directly alongside their medical student peers. For both, as well as the scientific community at large, the boutique program at the University of Southern California (USC) linking engineering and medical training at the graduate level is instructive of a new way of approaching engineering education that can potentially provide benefits to both students and society. Students who have grown up in an era of “mass customization” in the retail and service industries can enjoy that same degree of flexibility also in the realm of education. At the same time, society gains engineers who have developed an increased empathy and awareness of the clinical contexts in which their innovations will be implemented.
The aim of this article is to describe the lessons learned since the establishment of the Health, Technology, and Engineering Program at USC (HTE@USC) in 2011. The program was designed to each year enable a group of twelve highly motivated students, working in teams, to learn about and to participate in all phases of medical device development. It admits engineering students from across different departments of the Viterbi School of Engineering who have completed their first year of graduate coursework doctoral studies. Medical students are selected from applicants who have been admitted to the Keck School of Medicine and who have expressed interest in adding the program. All student applicants are interviewed to assess their level of motivation and commitment since program involvement of four years or more could mean an added year in school for students from either school.
A key feature of the program is that the engineering students take a year of the Introduction to Clinical Medicine (ICM) course that is the foundation of the medical education received by every trainee of the Keck School of Medicine. Diagnostic interviewing and the basic components of the physical exam are learned and practiced in clinical settings. All HTE students are jointly supervised and trained by clinicians committed to the HTE@USC aim of boosting empathy and awareness of clinical work. Engineers graduating with the HTE@USC graduate certificate have lived in the shoes of their medical student counterparts and have an enriched perspective. The ICM training instills an appreciation of the context as well as interpersonal skills that greatly enhance the ability of these students to interact with clinicians and health administrators with greater appreciation, confidence, and authenticity.
The hope is that now that four cohorts have started the program and the first graduates will soon have completed it, key components in the success of the program can be shared with others who may be considering creating a similarly tailored program.
Lesson One: Predictably Unpredictable
Training people seeking to develop the diverse skill set needed to create, test, and commercialize health care solutions, predictably, has proven to be nonlinear, iterative, and often unpredictable. Doing so in an academic context requires flexibility in multiple dimensions. Practices, scheduling, priorities, and outcomes are just a subset of these dimensions. For practices, for example, medical students routinely are funneled through the paperwork, tests, and scans required to get access identification badges. The addition of Ph.D. students has required additional instruction and guidance for both students and hospital administrators such that the process takes longer as a result. The steps required to gain access to health facilities vary between private hospitals, state facilities, and pediatric care sites. Tested knowledge of the Health Insurance Portability and Accountability Act (HIPAA) compliance rules, tuberculosis tests, and other medical clearance requirements are all mandatory. Physician tutors of the ICM, required of all medical students and also the graduate engineering students in the HTE program, tailor their choice of clinical sites based on access available to the students in their six-person groups. A variety of clinical sites provide the greatest breadth of both instruction and observation, ensuring all students have a wide range of experience as more sites become open to students over the course of the year. The freedom to travel across different clinical, university, and lab settings enables the students to act as the glue that connects different people and groups across these contexts.
Customs and culture vary between the two schools even at the same university. USC medical students spend most of their time at the Health Sciences Campus located eight miles from the University Park Campus, with downtown Los Angeles in between. In the first year of HTE, students have classes on both campuses and become familiar with the resources available at each site. The camaraderie that naturally develops is enhanced through assignments requiring the Ph.D. and M.D. students to pair off for shadowing clinicians, interviewing hospital staff, and observing in clinical sites. Individual, pair, and larger team projects are tailored to blend the curriculum readings and topics with activities coordinated with clinical departments. Students hear from and interact with a variety of guest speakers who represent different disciplines, clinical specialties, technology backgrounds, and relevant content expertise (e.g., conducting marketing assessments for medical devices).
In the university context, flexibility can be difficult since systems are in place to ensure that programs of study leading toward degrees and certificates are linear and predictable. New programs tend to be granted a bit of latitude before core content, options, and timing become more or less fixed. In developing the HTE@USC curriculum, requirements of both engineering and medical accreditation bodies are established and must be maintained. HTE’s added course content is necessarily supplemental and is designed to include a regular active learning component that helps to keep motivation high and attention focused. Flipped classroom approaches allow students to engage in an iterative learning-doing process that maintains motivation in at least two different ways. Since students have an active, intentional role in articulating the medical need they are currently working on, they are driven, for example, to use effective creative tools to generate possible solutions, to gain deeper relevant clinical knowledge, and, in intellectual property parlance, to search for prior art that might impinge on their freedom to operate based on a particular solution. Each of these “just-intime” knowledge sets is applied—and reapplied as necessary— on projects undertaken during the first year in the HTE projects. As the year progresses, “mini-projects” of increasing complexity and added layers of consideration are completed by students working in pairs.
Lesson Two: Clinical Context Influences Motivation
As is described in this article, at another level, each of the miniprojects is embedded in a clinical context that also positively influences motivation. External recognition, input, and guidance toward selecting projects that should continue come from the department or unit in which the clinical need was articulated. Sometimes this begins with a list of needs generated by clinicians. Whether the chosen need comes from clinicians or, in other exercises, from their own observations, students must reformulate it to generate the widest range of solutions in which unpredictable solutions are to be celebrated. External motivation also comes via the task of finding engineering faculty members whose expertise could be helpful in addressing the need that, in its rearticulated form, poses a challenge that arouses their interest.
We sometimes call these “catch-and-release” projects. In cases where the HTE students catch the attention of other students and their faculty mentors, they are encouraged to release the projects to them. In one such case, a project using ultrasound technology to build an artery locator for infants was taken up by biomedical engineering undergraduate students who continued to develop the concept in a regulatory science class. As the concept evolved, some of these students continued to participate when it was used in a senior biomedical engineering course on prototyping. Students hopped on and off the project, and, one year later, the team that was on won a student innovation prize in a competition sponsored by the university’s technology transfer office. None of this was predicted. Rather than trying to replicate this instance and solely conduct repeated “catch-and-release” exercises, we have experimented with a range of mechanisms to advance projects where intrinsic motivation of a changing team of students is further fueled by external support through mentorship and competitions.
Lesson Three: Design Thinking Requires Empathy
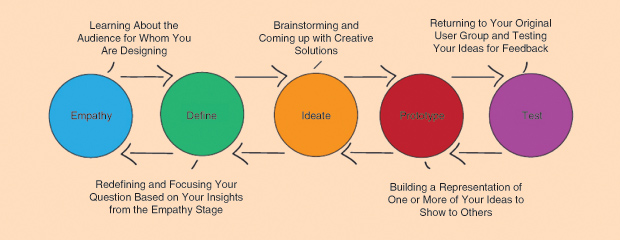
Empathy is at the heart of the definition of the design thinking process. Our aim in actively encouraging and cultivating empathy among our students is to foster a desire to continue to use and build empathic skills. The ability to understand and to accurately reflect back and share how people feel approximates the dictionary definition of empathy. Practicing these skills consistently in working on their increasingly complex projects, HTE students boost their empathy quotient. Design thinking is, more completely, a blend of empathy-inspired thinking that is necessarily action oriented. It requires purposeful research to deepen understanding that leads into applying other tools (such as brainstorming) to generate many potential solutions. This is depicted in Figure 1.
Students learn about design thinking and practice using tools from those developed by and routinely applied by designers. Early in the first semester of the program, HTE@USC students and invited guests learn and practice using a highly effective Design Thinker workshop, which also whets appetites for applying the tool kit in planning and conducting their projects.
The first axiomatic lesson taught in the HTE@USC program is that recognizing and articulating a need are at the core of a designer’s application of empathy. The lesson we’ve learned from the students is that, when it comes to empathy, they will either use it or lose it. To tip the balance toward use, we’ve learned to remind students via exercises explicitly structured for this purpose. As outlined previously, whether needs are observed or solicited from clinicians or other health care workers, activities across settings should require students to practice articulating needs. Presentations with slide decks structured so that students share and reflect on what design thinking tools they used to spark their creative solutions are scheduled at least twice per semester.
Design thinking also places a high value on generating many ideas. A tool kit of activities that help with this is very useful to aspiring medical innovators. Tactics to promote divergent thinking (we use the book Gamestorming: A Playbook for Innovators, Rulebreakers, and Changemakers) and rules that facilitate productive brainstorming sessions (as outlined in Stanford’s textbook Biodesign: The Process of Innovating Medical Technologies, 2nd edition) help students, as part of different projects, produce a variety of solution concepts. With repeated practice, ease of generating and prioritizing different solution concepts and applying filters (e.g., market considerations, anticipated regulatory hurdles, and reimbursement options) is developed. This, in turn, provides a helpful foundation for a willingness to propose and test different potential business models and ability to “pivot” (in the parlance of the Business Model Canvas).
Lesson Four: The Importance of Getting Feedback from Prototypes
Taking rudimentary prototypes and getting direct, physically inspired feedback—both observed nonverbal observations as well as verbalized responses—from a diverse set of stakeholders are both critical for medical devices. The more channels of feedback, the better. At this early stage of product development, students must be reminded that the aim is not to get a list of desirable features but rather to hone their offering down to a minimum viable product. Free-hand sketches shared with clinicians and engineers are a good starting point. Students with computer-aided design experience should be discouraged from investing too much effort during this phase. The risk, again, is that the students, by investing their time and effort in preliminary designs, may find it difficult to abandon them and start afresh. This willingness to experiment and to be open to unforeseen results also has to be practiced and rewarded. A foam-core “low-resolution prototype” can yield valuable insights worth the cost of experiencing the pain of letting go of ideas that seem perfect in the eye of the creator.
Lessons about and from experiments with prototypes extend beyond physical prototypes. The current boom in online offerings focused on user-interface experience and design for app development illustrates this point. As apps proliferate, key differentiators include such aspects as stickiness, intuitive ease-of-use, customization features, visual beauty, etc. For medical apps focused on facilitating patient engagement through two-way information sharing, the experience of patients using the app can easily trump the content focus of the app. In a student project in which an app was developed to solicit patient feedback about aspects of their care experienced in an emergency department setting, lowtech texting was sufficient to gather and prioritize patient needs, leading to real-time corrective actions by hospital staff members. Project Empath led to an unforeseen opportunity to rescue potential service failures by taking the pain out of parking; for example, see this story.
Lesson Five: Iterating, Iterating, Iterating
What location is to real estate pricing, iterating is to innovation. In addition to the benefits previously outlined, iterating also has the indirect positive effect of decreasing the fear of acting and allowing team members to learn more from unanticipated outcomes generating the action portion of the empathy loop. Beginning with paraphrasing their understanding of the thoughts and feelings of an interviewee, students learn how to fine-tune and develop their empathy. After repeated trials, when practiced tactfully and reflectively, students display fewer inhibitions around asking empathically attuned questions and making insightful observations. Such inhibition is often attributed to fear of anticipated failure when, as inexperienced practitioners, students try to intuit how someone feels. Fear of failure in this microlevel sense can also be connected to a generalized inhibition toward stating and checking interpersonal hypotheses. One can only overcome such a fear by experiencing failure to intuit someone’s feelings and thoughts by building a conviction to learn from the improved perception feedback on verbalized “guesses” solicits. Very bright students who are accustomed to being correct are very good at being defensive and deflecting such feedback.
Using the goal of improving empathic skills is thus a very useful method of teaching people how not to fear failure. This has the double benefit of enabling students to understand needs better at a basic level while learning how to generate hypotheses and test them interpersonally. This is an action-oriented form of learning that becomes very useful as students begin to address other components of the business model canvas after the initial focus on customer development. Students learn to practice making hypotheses regarding other business model considerations and do so more accurately because of the openness to corrective feedback and confidence in an iterative approach they’ve developed in the crucial phase of customer development.
Lesson Six: The Importance of Interdisciplinarity
Learning each time you iterate can be enhanced through interdisciplinarity. By sharing feedback among a team consisting of members representing different professional disciplines, students have the added opportunity to listen through the ears of different communities. Each community, as represented in student team members and mentors, can offer different, complementary interpretations of perceived feedback. Openness to bringing multiple perspectives into the construction of a new, common understanding is an essential differentiator of an interdisciplinary versus a multidisciplinary team.
In the HTE program, M.D. students don’t have to come from an undergraduate engineering program. As successive classes have demonstrated, almost all who haven’t had it want more engineering training. Wanting to understand the language and practice of engineering more deeply is likely a side effect of emphasizing the importance of appreciating multiple perspectives. Medical students are now encouraged to take engineering courses—or components of courses—attuned to their team project. The overriding aim is to maintain positive, milestone-driven progress on the team’s project. Students should be incentivized to see that it is less important to take courses toward an individual degree than it is to get “just-in-time” skills and knowledge to keep a project going and the team productive. Some students seek a break from medical studies to participate more fully on their team projects. Those students who have done so already have also found enough extra time to participate in multiple projects. Those who successfully juggle multiple projects will have a portfolio of accomplishments by the time of graduation. Among those who are very successful, we anticipate that a few may even opt to build companies founded on their technology rather than graduating from either the M.D. or Ph.D. program.
Lesson Seven: Give Students the Opportunity to Compete for Financing
As mentioned previously, there is no shortage of opportunities for students to compete for funding and access to resources such as legal assistance. External funding opportunities also help teams focus on continued product development and improving their presentation skills as they learn more about business concepts they will need to start and build their companies. Competitions build a sense of urgency about learning these concepts. HTE students have been successful in businessplan competitions, accelerator/incubator applications, and Small Business Innovation Research Program grant applications. Since the deadlines and rules are not connected with inclass deliverables and sometimes conflict, flexibility is needed to accommodate student extracurricular activities. One practical approach is to use them as options within a “flipped-classroom” course format that can substitute for class-prescribed activities.
These lessons are meant to encourage replication, discussion, and collaboration across institutions seeking to foster similar programs. While HTE@USC may take a while to see a project offshoot of blockbuster proportions, the creativity unleashed by daring to ask “What if?” in the context of talented teams focused on medical issues has launched projects that have had impact. The range of ideas itself has been exciting: from applications using a novel antimicrobial surface coating to a speedy bonemarrow extraction device designed for use with a local anesthetic for donors who will experience far less pain than donors do now. In the longer term, we expect many novel projects from our graduates. Our hope is to equip our students to become lifelong empathic entrepreneurs.