
Just before the COVID-19 pandemic, 2019 marked the 100th anniversary of the school and manifesto of the Bauhaus. Now that life is slowly returning to normal, it may be a good moment to celebrate one of the most transformative educational initiatives ever, with the motivation of developing a model that could also transform BME.
The Bauhaus model and contemporary engineering education
The Bauhaus was founded by Walter Gropius in 1919 with the intention of linking architecture with design and allowing art to merge into industry. The Bauhaus’ remarkable professors—Johannes Itten, Paul Klee, Wassily Kandinsky, Oskar Schlemmer, Lyonel Feininger, László Moholy-Nagy, and Gropius himself—were relevant representatives of a truly singular generation of designers, architects, and artists. In the less than 15 years it existed, the Bauhaus transformed the worlds of architecture and product design and achieved long-lasting global impact through its hands-on training [1].
Modern engineering education has progressively incorporated learning by doing as fundamental for professional development and for learning how to deal with complex multifaceted problems. In Europe, the transition to the European Area of Higher Education has sparked student-centered methodologies like problem-, challenge-, project-, and game-based learning. Worldwide, the conceive design implement operate (CDIO) initiative is transforming engineering education through holistic project-based learning (PBL) [2]. It is important to point out that this was already present in the Bauhaus model one century ago, although the Bauhaus did not last enough to change higher education worldwide.
“Biomedical Bauhaus” as transformative model for future “health engineering” campuses
In connection to health care technologies, most accredited BME programs and successful approaches to hands-on BME training also rely on PBL actions. Mainly they focus on technology development and entrepreneurship, which is adequate for creating successful professionals for high-tech companies, but possibly not broad scoped enough for true societal transformation. In fact, health care technologies have only a limited impact on human health, which should be approached more globally, as the “one-health” concept from the World Health Organization (WHO) points out [3], following pioneering principles from Acheson’s team report [4].
Indeed, infrastructures, hospitals, clinics, primary care centers in rural areas, processes and supply chains for medicines, machines for clean water, appropriate food technology—among other aspects—influence health at least as great as biomedical technology. Nevertheless, they are seldom tackled in BME courses and programs, as schematically represented in Figure 1.
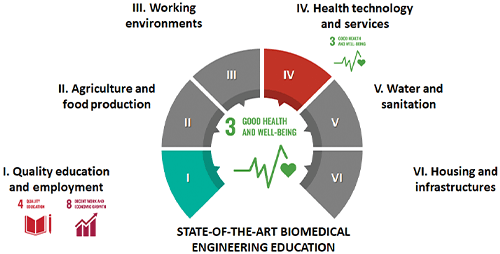
Figure 1. Scheme of health dimensions covered in state-of-the-art BME programs, usually focusing on health care technologies and quality education for promotion of employability. Health dimensions adapted from Acheson’s report [4]. Cycle template by PresentationGo.
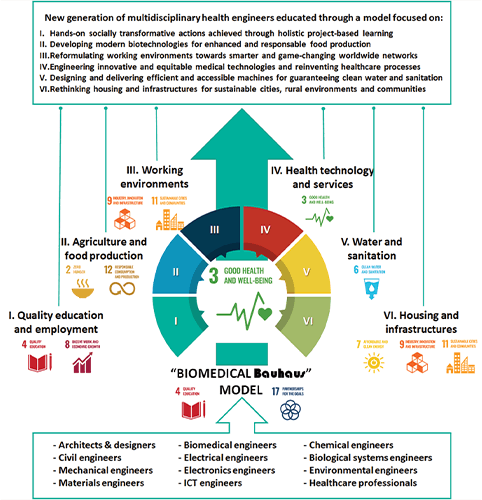
Figure 2. Schematic of biomedical Bauhaus model: training a multidisciplinary cohort of engineers for approaching health globally. Cycle template by PresentationGo.
The ideal training for these health engineers would resemble the Bauhaus model in many ways, especially for its holistic training of architects and artists capable of approaching all kinds of designs and transferring them to society to make an impact. Of course, the Bauhaus model should be reformulated to nurture a new generation of multidisciplinary engineers and synergic specializations managing health care and health technologies with a true global perspective focused on one-health.
These biomedical Bauhäuser models should expand through globally connected clusters or campuses to make true impact, forming a unique global university that would apply other principles from the original Bauhaus, apart from its holism. Campus life would be central to the learning strategy. Constructing the campus as a way of learning, considering the campus as part of urban and rural life for improving health, taking advantage of the campus design for involving the community, and searching for user-centered solutions, would make this educational experience unique. Besides, the “form follows function” principle would also play a central role, both at a technology level for enhanced interactions with the human body, and at an infrastructure and ecosystem level, for reaching organic or bioinspired construction and organizational models, through which the educational scheme would be sustainably deployed.
The most relevant: students and educators would work as a single multidisciplinary team with global impact to transform health through educational practice and its results. CDIO-style PBL could be the applicable teaching-learning methodology, adequately supported by co-creation environments and platforms conceived for sharing results and expanding the model. Ideally, projects would be open source but not necessarily free, probably quite the opposite, as reaching market with developed technologies, designs, methods, and infrastructures, would make the model economically sustainable and promote increased societal impacts. Topics for biomedical Bauhaus’ projects and products to structure the learning process through project-based actions and make the model sustainable through societal impact include:
- Innovative hospitals and reinvented health management processes.
- Prefabricated and modular designs for primary health care centers.
- Infrastructures for healthy and smart cities and villages.
- Healthy buildings and environments.
- Machines for healthier lives including machines for sports practice.
- Technologies and infrastructures for clean water.
- Technologies and processes for healthy food growing and processing.
- Manufacturing hubs for point-of-care medical devices.
- Innovative health care technologies for prevention, diagnosis, monitoring and treatment.
- Spin off and startup companies based on previous technological advances and inventions.
Personalized approaches to health care, artificial intelligence-aided products and processes, point-of-care manufacturing and testing, as well as co-creation actions among international cohorts are among the trends that would be fostered throughout the educational model, working towards increased cooperation and equity. The internationalization of students and educators through innovative mobility programs would reinforce the desired collaboration across campuses and countries.
Challenges and action plan: a model for transforming health through holistic education
First programs of studies following the biomedical Bauhaus model still need to be designed in detail and implemented. The schemes of Engineering Education 5.0 [5], as an organizational complement to make the model operative, could be employed. For a successful and equitable implementation, it should not be a university for the privileged or driven by private initiative, but a public campus open to all based on merit, following Article 26 of the Universal Declaration of Human rights.
An international advisory board should support its design, with health researchers, health care professionals, philosophers, and ethicists playing a key role in the implementation and supervision of programs. In general, the “health as business” concept should be avoided, while the long-lasting dream of health care accessibility should be pursued [6]. Ethical discussions on the desire for healthier societies and their eventual implications on individual freedom should be wisely and carefully addressed, to avoid pursuing a healthy utopia with ranked or segregated citizens and technoscientific domination [7]. Space for ethical debate should be fostered through curricular activities and reinforced through extracurricular actuations, connecting with applications of Habermas’ theory of communicative action to education [8].
A pilot project with one biomedical Bauhaus operating by 2030 and acting as exemplary seed, with a first cohort of health engineers by 2035, and ten working replicas with cohorts of alumni already by 2040, would be a realistic temporal framework for implementation. Political long-term compromise is needed, to avoid a commercialization of the model and to prevent the “health as business” concept from corrupting the path toward a new type of engineer acting as health sentinel. To this end, simplified accreditation schemes, considering the singular nature of such a proposal, and the generous commitment of colleagues from different fields, avoiding battles of egos, would also be pivotal.
In conclusion, it is not the moment for sterile discussions about the frontiers between BME and medical physics, but a time for finally tearing down borders among scientific and technological fields, for creating a new generation of multidisciplinary professionals who would be health engineers with the ambition of synergically contributing to improved health worldwide. The biomedical Bauhaus model schematically proposed here will hopefully support or help to inspire these desired transformations, connecting SDGs 3 on “Good Health and Well-Being” and 4 on “Quality Education” in unprecedented ways.
The debate is open. Let’s dare to take the first step.
References
- M. Droste, Bauhaus: 1919-1933. Cologne, Germany: Taschen, 2019.
- E. Crawley et al., Rethinking Engineering Education: The CDIO Approach, 2nd ed. Cham, Switzerland: Springer, 2014.
- World Health Organization. (Nov. 1, 2022). One Health Initiative. [Online]. Available: https://www.who.int/teams/one-health-initiative
- D. Acheson, Independent Inquiry Into Inequalities in Health Report. Richmond, U.K.: HMSO, 1998.
- A. D. Lantada, “Engineering education 5.0: Continuously evolving engineering education,” Int. J. Eng. Educ., vol. 36, no. 6, pp. 1814–1832, 2020.
- World Health Organization, “Declaration of Alma-Ata,” in Proc. Int. Conf. Primary Health Care, Alma-Ata, USSR, Sep. 1978, p. 3.
- A. Asai et al., “Should we aim to create a perfect healthy Utopia? Discussions of ethical issues surrounding the world of project Itoh’s harmony,” Sci. Eng. Ethics, vol. 26, pp. 3249–3270, Oct. 2020.
- M. Murphy and T. H. Fleming, Critical Theory and Education (Routledge International Studies in the Philosophy of Education). Milton Park, U.K.: Routledge, 2010.